From the Editor
The world changed on March 11, the day that the pandemic was declared by the WHO. So did mental health care, with so many of our services becoming virtually delivered. But what’s effective and what should be incorporated into care moving forward?
This week, we have three selections.
The first is a new JAMA Psychiatry paper. With COVID-19, apps are becoming increasingly popular (one therapy app reports a 65% increase in clients over the spring). Can the apps be incorporated into primary care? Andrea K. Graham (of Northwestern University) and her co-authors do a RCT using apps for patients with depression and anxiety. They conclude: “In this trial, a mobile intervention app was effective for depression and anxiety among primary care patients.” But should we be so enthusiastic? And how could apps be used in care?

Canada legalized cannabis for non-medical purposes in 2018. In a short research letter – our second selection – medical student Laura A. Rivera and Dr. Scott B. Patten (both of the University of Calgary) consider driving under the influence of cannabis, drawing on national survey data. “Public policy actions toward prevention of DUIC [driving under the influence of cannabis] appear necessary and will have the greatest impact if they are effective in the 15 to 24 age range and in males.”
Finally, in the third selection, we consider an essay from The Globe and Mail. Like many, Vera Oleynikova thinks about the return to school. She writes about her own experiences, noting a complication: she has struggled with depression. “To be sick for a long time and then to feel well again is a magical thing. You feel brand new and capable of anything. You marvel at your own capacity to do the things that for a long time were unavailable to you because of your illness. Which is why going back to school at 31 felt so right.”
DG
Selection 1: “Coached Mobile App Platform for the Treatment of Depression and Anxiety Among Primary Care Patients: A Randomized Clinical Trial”
Andrea K. Graham, Carolyn J. Greene, Mary J. Kwasny, Susan M. Kaiser, Paul Lieponis, Thomas Powell, David C. Mohr
JAMA Psychiatry, September 2020

Depression and anxiety are prevalent, impairing, and costly health problems, most often treated in primary care. The US Preventive Services Task Force recommends routine depression screening in primary care; however, without additional assistance to support treatment, increased identification provides no benefit. Unfortunately, demand for mental health services outweighs workforce capacity and resources to meet these needs. Digital mental health interventions (DMHIs), using Internet-based and mobile tools, can be cost-effective and have potential to improve capacity of health care settings to address mental health problems. However, implementation in primary care has often failed, primarily because patients do not use the tools.
Computer-delivered DMHIs are primarily based on evidence-based therapies, rely heavily on psychoeducation, and typically require use for 30 to 45 minutes per week for 6 or more weeks. Despite good efficacy in randomized clinical trials (RCTs), real-world engagement is challenging. In contrast to computers, people tend to use smartphone apps for a single purpose, in short bursts of time, sometimes frequently throughout the day. Thus, app-based DMHIs often focus on 1 to 2 psychological strategies and more on actions than psychoeducation. App-based DMHIs have demonstrated efficacy in RCTs, are increasingly used by the public, and produce reasonable early engagement, but adherence drops dramatically over the first 2 weeks.
App-based DMHIs may have greater success if they accommodate app use conventions and overcome 2 major challenges for delivering mental health interventions. First, the many effective behavioral strategies may appeal differentially to different people. Second, people do not tend to use mental health apps for long periods. This may be because people seek the novelty of new apps or have acquired the app’s benefit and no longer find it useful. Thus, a single app approach for a mental health condition may be less effective.
So begins a paper by Graham et al.
Here’s what they did:
- Using a RCT, they compared a digital platform, IntelliCare, with wait list control for people with depression and anxiety.
- Participants were primary care patients of the University of Arkansas for Medical Sciences (UAMS). They were recruited between July 17, 2018, and December 14, 2018.
- Inclusion criteria: “elevated symptoms of depression or anxiety at screening (score ≥10 on the Patient Health Questionnaire-8 or ≥8 on the Generalized Anxiety Disorder-7 scale)”; exclusion criteria included suicidal thoughts.
- They were randomized to the intervention or they remained on wait listed control, but have the intervention after 8 weeks. (!)
- Re: IntelliCare. “Rather than a single app, the platform contains multiple apps, each of which is brief, simple, and supports a single clinical target. For example, the Daily Feats app targets goal-setting; the sole activity is setting and monitoring completion of daily goals, with scaffolding to increase complexity.” They had access for 8 weeks, and were coached.
- Statistical analyses were done.
Here’s what they found.
- 146 patients were included.
- Demographics: 119 of the 146 were women (81.5%). The mean age was 42.3 years. 122 (83.6%) were diagnosed as having depression and 131 (89.7%) were diagnosed as having anxiety; many had both.
- Most (96.6%) completed at least 1 follow-up session.
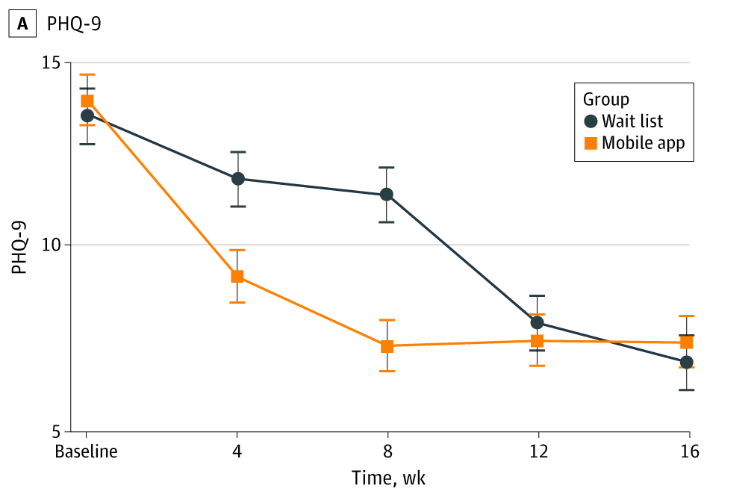
- A greater proportion of intervention vs. wait list control participants achieved recovery from depression (59% vs. 31%) as well as for anxiety (57% vs. 38%). “Sustained effects were observed for depression (slope, 0.01…) and anxiety scores (slope, 0.02…) during follow-up.” See graph below.
“This is, to our knowledge, the first RCT of an app-based platform for the treatment of depression and anxiety and of any app-based mental health treatment among primary care patients. Individuals who received the mobile platform had a greater reduction in depression and anxiety symptoms compared with treatment-as-usual WLC individuals, and changes were sustained over 2-month follow-up.”
A few thoughts:
- This is a good study – a well-designed RCT.
- This is a timely study. As we begin to consider our digital moment, the authors provide evidence for an intervention that works.
- There is much to like here from a health systems perspective. Apps aren’t particularly expensive; though the study provides no costing, it seems reasonable to assume that the intervention wouldn’t be particularly costly – especially compared to the economic burden of depression and anxiety.
- Are the results too good to be true? One limitations here: the majority of patients (56%) were on medications, which could have affected results.
- So should we suggest apps to our patients? There is evidence that some respond to the interventions of apps. It should be noted, however, that apps can be downloaded but not really used (Baumel et al. found that 96% of people didn’t use popular mental health apps after two weeks). This study had two coaches who texted patients encouraging them to use IntelliCare. So suggesting an app to a patient in your practice may not yield these robust results. And it’s tough to pick apps given how many have been developed. One option: the American Psychiatric Association now has an App Advisor with advice on choosing apps, and a growing library of apps that are evaluated using a simple, practical evaluation tool. You can find it here:
https://www.psychiatry.org/psychiatrists/practice/mental-health-apps
The full JAMA Psychiatry paper can be found here:
https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2766444
Selection 2: “Driving Under the Influence of Cannabis in Canada, 2015 to 2018”
Laura A. Rivera and Scott B. Patten
The Canadian Journal of Psychiatry, September 2020

Legalization of nonmedical cannabis occurred in Canada in October 2018, necessitating a stronger understanding of potential consequences such as driving under the influence of cannabis (DUIC). Evidence associating DUIC with increased risk of motor vehicle collisions stems from natural experiments upon cannabis legalization, simulation research, and linkage studies to actual crash data. To augment this knowledge base, relevant items have been included in recent population-based surveys in Canada.
So begins a research letter from Rivera and Dr. Patten.
The paper drew from two national databases: “We analyzed cross-sectional population-representative data collected by the Canadian Community Health Surveys (CCHS) from 2015 to 2018 and the Canadian Tobacco, Alcohol and Drugs Survey (CTADS, 2017).”
Some findings:
- “For all 4 years, the highest rate of DUIC was that for males aged 15 to 24, where the frequency ranged between 20% and 40% of cannabis users.”
- “The lowest frequency was in women aged 25+, where the prevalence ranged from 7% to 17% of those reporting cannabis use.”
- “In aggregate, these frequencies represent approximately 2% to 3% of the population in each year.”
- “In our analysis, males aged 15 to 24 were consistently found to have the highest prevalence of DUIC. As a group, young males are more likely to engage in risk behaviors including drug use compared to other groups. Higher rates of DUIC were noted in Alberta compared to Ontario although the estimates were insufficiently precise to fully confirm this. ”
The authors suggest that public policy efforts focus on young men.
A few thoughts:
- This is a short research letter – but it offers new and important data.
- The policy prescription seems quite practical.
- What to make of the numbers? 2-3% of people driving under the influence of cannabis is significant. Are the numbers going to change with time as people grow more accepting of cannabis? Will they drop, as public education campaigns inform?
- And how should we change our patient interactions? We ask patients about cannabis use – should we also ask more explicitly about driving and cannabis?
The research letter can be found here:
https://journals.sagepub.com/doi/full/10.1177/0706743720922655
Selection 3: “When my depression lifted, I had the confidence to start over at school”
Vera Oleynikova
The Globe and Mail, 3 September 2020

By age 30, I had an unfinished degree in English cultural studies, finger knuckle tattoos and no resume. I had spent the last six years cashing in government cheques for a disability that ranged from benign to totally debilitating, depending on the day. I had no discernible skill set yet had somehow managed to convince a local theatre company that I was the right person to handle props for an upcoming production.
Impressed by my sheer gumption and can-do attitude (or else, unable to find any qualified person willing to work for so little pay), they invited me back. That one props gig led to more and eventually other theatre companies began reaching out to me as well. Props requests turned into: ‘Hey, we need someone to do sets …’ or ‘Can you do costumes?’ ‘Sure!’ I said, having not the slightest clue how to do any of those things.
For the first time in my life people were offering to pay me money to do something other than the most menial tasks. And I figured it would probably be a good idea to be at least a little bit qualified at that thing I was being paid to do.
So begins an essay by Oleynikova.
She writes about the challenges of returning to school:
“Being in school in your 30s means you are old enough to know what you want and how to go after it. The work itself is relatively easy after having to navigate life as an adult, and your professors make great intellectual sparring partners and usually happen to be nice people who like their jobs. But being in school in your 30s can be depressing, too, because – let’s face it – you are in school in your 30s.”
She also discusses her mental illness:
“My first shot at university was defined as much by mental illness as by a persistent feeling of ‘what am I doing here?’ It took a herculean amount of effort to get out of bed and make it to my 8 a.m. classes as I wondered, did I really need to know what a Marxist theorist thinks about Sex and the City? And what would I do with that after graduation? The future was one big scary unknown, marred by the lingering suspicion that I actually wasn’t cut out for any sort of employment, period. My depression clouded my brain like a heavy haze. I’d think to myself: is this really who I am? This terribly uninteresting person with nothing to say who is barely making it? It wasn’t until my late 20s, when I started taking antidepressants, that I began to know my true self, who is as smart and funny and competent as anyone.”
She closes:
“Despite everything, it feels like, 12 years later, I am finally getting undergrad right.”
A few thoughts:
- This is a great essay.
- We should marvel at her courage – of going back to school, yes, and also in speaking so candidly (and publicly) about her mental illness.
- What a great story of illness and recovery. Two decades ago, when I told a close friend that I had matched to residency training in psychiatry, he responded: “what happened?” Though stigma still exists, Oleynikova’s essay reminds us of the importance of our work. That’s helpful to remember today, World Suicide Prevention Day, and every day.
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments