From the Editor:
“He’s here again.”
The staff would roll their eyes. Harold was back. Many of us had encountered him – a person with alcohol use disorder who frequently came to the emergency department of the hospital where I did my internship year. He would usually get a sandwich and a lecture. But what are the outcomes for people like him? And what could be done?

In the first selection, we consider a new CMAJ paper. Dr. Jennifer Hulme (of the University of Toronto) and her co-authors study outcomes for those presenting to Ontario EDs for alcohol-related reasons. The major finding: “The all-cause 1-year mortality rate was 5.4% overall.” We review the paper and its implications.
In the second selection, we look at a new essay by Dr. Rebecca Lawrence from The Guardian. The UK psychiatrist, who has written about her experiences as a mental health patient, notes the challenges of psychiatric diagnoses. “There are many words in the field of mental illness that have been discarded and are now viewed as stigmatising and inappropriate – words such as ‘cretin’, or ‘lunatic’, or ‘mental’. It’s interesting to consider whether our current crop of acceptable words will end up in that category, and it’s salutary to know that many probably will.”
DG
Selection 1: “Mortality among patients with frequent emergency department use for alcohol-related reasons in Ontario: a population-based cohort study”
Jennifer Hulme, Hasan Sheikh, Edward Xie, et al.
CMAJ, 23 November 2020

Alcohol is a leading driver of morbidity and mortality worldwide. An estimated 3 million deaths in 2016 – 5% of all global deaths – were attributable to alcohol consumption. The 2016 Global Burden of Disease Study showed that alcohol was the single greatest risk factor for ill health worldwide among people aged 15–49 years. In Canada, hospital admissions for alcohol-attributable conditions out-number those for myocardial infarction. Alcohol-related harms cost Canadians about $14.6 billion annually, with $3.3 billion in health care costs.
In addition to the societal impact of mental and behavioural disorders due to alcohol (henceforth referred to as alcohol-related) – mainly acute intoxication and withdrawal – these disorders are common reasons for emergency department visits. Data from the United States and Canada, furthermore, suggest that alcohol-related emergency department visits have increased in recent years. For example, a study in Ontario showed that, between 2003 and 2016, the age-standardized rates of alcohol-attributable emergency department visits increased by 86.5% in women and 53.2% in men. People who visit emergency departments frequently for alcohol-related reasons have high levels of comorbidity and social disadvantage, and represent a readily identifiable patient population for whom interventions to address unmet social and health care needs could be developed. A systematic review suggested that screening and brief intervention for alcohol-related problems in the emergency department is a promising approach for reducing problematic alcohol consumption.
Despite this, little is known about the risk of death, a key outcome for health system performance, among people who use emergency departments frequently for alcohol-related reasons, including whether mortality risk increases with increasing frequency of visits. To address this gap, our primary objective was to describe the sociodemographic and clinical characteristics of this high-risk population and examine their 1-year overall mortality, premature mortality and cause of death as a function of emergency department visit frequency in Ontario, the most populous Canadian province.
So begins a paper by Hulme et al.
Here’s what they did:
- “We conducted a retrospective population-based cohort study of all residents aged 16–105 years in Ontario (population 13.5 million in 2016) who made frequent emergency department visits for alcohol-related reasons between Jan. 1, 2010, and Dec. 31, 2016.”
- They drew data from several databases including the National Ambulatory Care Reporting System (for ED data), and the Canadian Institute for Health Information Discharge Abstract Database and the Ontario Mental Health Reporting System (for hospital admissions).
- They considered those who made at least 2 emergency department visits for mental or behavioural disorders due to alcohol within 1 year.
- “The primary outcome was all-cause mortality 1 year following the index alcohol-related emergency department visit.”
- Statistical analyses were done.
Here’s what they found:
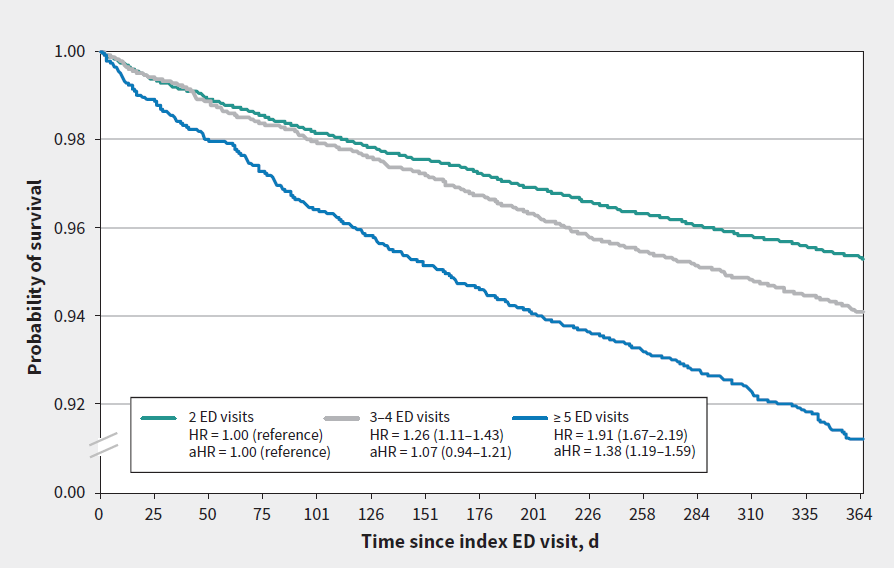
- “Of the 25 813 people included in the cohort, 17 020 (65.9%) had 2 emergency department visits within 1 year, 5 704 (22.1%) had 3 or 4 visits, and 3 089 (12.0%) had 5 or more visits.”
- Those with 5 or more visits tended to be males, people aged 45–64 years, those living in urban centres and those living in lower-income neighbourhoods.
- The all-cause 1-year mortality rate was 5.4% overall with a range: from 4.7% among patients with 2 visits to 8.8% among those with 5 or more visits.
- “Death due to external causes (e.g., suicide, accidents) was most common.”
- “The adjusted mortality rate was 38% higher for patients with 5 or more visits than for those with 2 visits (adjusted hazard ratio 1.38, 95% confidence interval 1.19–1.59). Among 25 298 people aged 16–74 years, this represented 30 607 YPLL.”
A few thoughts:
- This is a good study.
- Ouch.
- To repeat: “The all-cause 1-year mortality rate was 5.4% overall with a range” – or about one in 20.
- How do the findings compare to other studies? “We observed a standardized 1-year mortality rate of 5.4%, which was higher than the 1-year mortality among Dutch patients admitted to intensive care units with alcohol intoxication (4.4%). The mortality rate we observed in the highest-frequency group, 8.8%, is comparable to the rate among patients admitted with myocardial infarction in a French study and is nearly 4 times the rate among people with 5 or more emergency department visits for any substance use in Alberta, 2.3%.”
- What’s to be done? “Frequent visits to the emergency department represent opportunities for timely intervention. Promising strategies include screening, brief intervention, treatment referrals, managed alcohol programs and case management. Rapid access to addiction medicine clinics has been shown to reduce both substance use and emergency department visits, and may also have an impact on mortality in frequent users of emergency departments for alcohol-related mental and behavioural disorders.” These recommendations go well beyond a lecture and a sandwich.
- This study is particularly relevant now, with evidence that alcohol use is up during the pandemic. In the last CAMH-Delvinia survey, more than one in four Canadians reported binge drinking within the last week. One of the lasting consequences of COVID could be more ED visits for alcohol-related reasons. Let’s hope we collectively do better.
The full paper can be found here:
https://www.cmaj.ca/content/192/47/E1522
Selection 2: “As both a psychiatrist and a patient, I know how slippery a diagnosis can be”
Rebecca Lawrence
The Guardian, 30 December 2020
![]()
Learning to be a psychiatrist means learning the names of a lot of disorders. Without these names, what would we have? A welter of distress, a confusion of symptoms. It would be very hard to say to a colleague, when pressed for time, what was wrong with any particular patient: ‘Well, his mood is low every morning, he doesn’t eat, his sleep is poor, his wife says he’s lazy and neglecting their child’ might only be the start. But if you say, ‘He has an episode of moderate to severe depression, not responding to an SSRI’, your average psychiatrist has a grasp of the problem and what they might need to do.
The problem is that the disorder, or the diagnosis, is attached to a standard group of symptoms and signs, which is fine if your patient fits them all neatly, but can be a problem if they don’t.
So begins an essay by Dr. Lawrence.
She notes the complexity of the illness experience:
“I learned about psychiatry from an external position of reading books, seeing patients and listening to those far more knowledgeable than I am. I experienced psychiatry in a state of fluctuating despair, with feelings of anger and self-loathing.”
She speaks of her own experiences:
“I have had my diagnosis changed a few times: from depression to bipolar disorder, back to depression and bipolar disorder again. I still find either hard to believe, and I think the changes have contributed to this. When I started writing and speaking more about being a patient, I asked my psychiatrist if he was going to change it again, at least partly because I felt I would lack credibility if this happened. He assures me he won’t, but the fact that it’s happened already means I can never fully believe him. I do believe I have some form of mental illness, but I’m still not sure it fits neatly into a box.”
She describes struggling with the importance of disease labels and recognizing their limitations. “So when I morph back into a psychiatrist, how can I marry the need to make diagnoses with my lack of personal commitment to them? I’m not sure I can. But I can try to accept that there are many things I won’t understand fully, and perhaps my own mental illness is one of these.”
She concludes: “So I will remember the names of these disorders and I will continue to use them, but I will remember that they are likely to change over time. This does not necessarily matter, and may reflect new thoughts, new concepts and, hopefully, new treatments. I will also remember the importance of these words for patients, and that they should not be lightly used.”
A few thoughts:
- This is a great essay.
- The core message is excellent: don’t forget to treat the patient, not just his or her diagnosis.
- DSM-5 is an inexact tool, allowing us reproducibility of diagnosis, but failing to allow for the richness of the individual.
- Dr. Lawrence has written about her experiences. In a previous essay, she writes about being a physician and a patient. “My career in psychiatry actually started on the other side, as a psychiatric inpatient going through multiple admissions, medications and courses of electroconvulsive therapy (ECT).” That essay was featured in a previous Reading, and can be found here: https://davidgratzer.com/reading-of-the-week/reading-of-the-week-trends-in-suicide-mortality-in-canada-cjp-also-suicide-prevention-quick-takes-and-lawrence-on-her-depression-guardian/
The Guardian essay can be found here:
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments