From the Editor
Can we nudge people to better choices? Economists, psychologists, and psychiatrists have all considered this idea. Though early work looked at pensions and finance, more recent studies in behavioural economics have considered topics in health care, like helping smokers quit.
This week, we open with a new paper that considers the concept of delay discounting in people with major mental illness. “Delay discounting” is a clunky term for the value that people place on rewards over time. Take two individuals, Paul and Peter, offered the same deal: they can be given $100 today or $200 in three months – Paul wants the $100 now while Peter is willing to wait for the bigger reward of $200. Paul, then, has more delay discounting than Peter.
Existing literature shows delayed discounting for people who have addiction and ADHD diagnoses. But what about others with mental disorders? McMaster University’s Michael Amlung and his co-authors study delay discounting by doing a meta-analysis, pulling data from 43 studies involving eight psychiatric disorders in this new JAMA Psychiatry paper. “To our knowledge, this meta-analysis is the first quantitative synthesis of delay discounting findings in psychiatric disorders, except ADHD and addictive disorders. This meta-analysis provides relatively strong evidence that delay discounting is a transdiagnostic process in psychiatric disorders.”
 Behavioural economics (and nudging): different for those with mental disorders
Behavioural economics (and nudging): different for those with mental disorders
In our second selection, we consider a longer essay on lithium for bipolar and its first champion. The University of Groningen’s Douwe Draaisma, a professor of the history of psychology, writes about urine, guinea pigs, and the beginning of the psychopharmacological era.
DG
“Delay Discounting as a Transdiagnostic Process in Psychiatric Disorders: A Meta-analysis”
Michael Amlung, Emma Marsden, Katherine Holshausen, Vanessa Morris, Herry Patel, Lana Vedelago, Katherine R. Naish, Derek D. Reed, Randi E. McCabe
JAMA Psychiatry, 28 August 2019 Online First
https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2749075
Examination of underlying neurocognitive processes that transcend multiple diagnostic categories is a long-standing priority in psychiatry. Consistent with this focus is the Research Domain Criteria (RDoC) framework from the US National Institute of Mental Health, which seeks to characterize the fundamental domains of cognitive, perceptual, and social processing with the aim of identifying novel targets for the treatment of mental health disorders. Within the RDoC framework, the behavioral economic index of delay discounting, which captures the extent to which rewards lose value over a temporal delay, has emerged as a promising paradigm. Delay discounting is commonly assessed through intertemporal choice tasks involving choices between immediate and delayed rewards (eg, money) to estimate a person’s discounting rate (k) or other quantitative indices (eg, area under the curve, impulsive choice ratio). Steeper delay discounting and, subsequently, smaller area under the discounting curve is frequently interpreted as reflecting an impulsive preference for immediate rewards over delayed gratification.
A growing body of research has solidified the relevance of delay discounting in the context of psychiatric disorders. This relevance has led to the proposal that excessive discounting of delayed rewards is a transdiagnostic process (ie, a behavior exhibited across multiple disorders that may provide novel insights into the common underlying features of those disorders). Furthermore, Levin et al proposed that investigating delay discounting across disorders may help inform transdiagnostic treatments by identifying target behavioral processes and providing markers of change in existing treatments.
 Michael Amlung
Michael Amlung
So begins a new paper by Amlung et al.
Here’s what they did:
- Searches were done using databases like PubMed, with studies up to 10 December 2018 using keywords from DSM IV and 5.
- Inclusion criteria included psychiatric diagnosis based on a validated diagnostic instrument. “Although a limited number of studies have assessed nonmonetary commodities (eg, food, effort), we focused on money as the most commonly and consistently assessed reward.”
- Studies selection was done through Covidence, with two co-authors independently screening the titles and abstracts.
- In terms of the meta-analysis: “Hedges g effect sizes were computed and random-effects models were used for all analyses. Heterogeneity statistics, one-study-removed analyses, and publication bias indices were also examined.”
Here’s what they did:
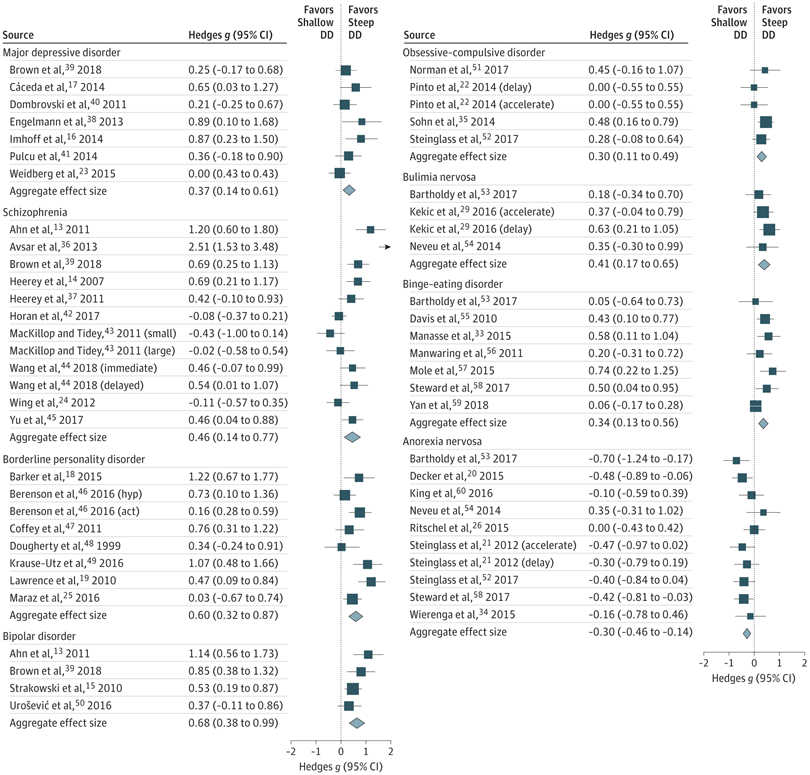
- “The sample included 57 effect sizes from 43 studies across 8 diagnostic categories.”
- Most disorders had steeper discounting for those than the controls.
- Specifically: major depressive disorder (Hedges g = 0.37; P = .002; k = 7), schizophrenia (Hedges g = 0.46; P = .004; k = 12), borderline personality disorder (Hedges g = 0.60; P < .001; k = 8), bipolar disorder (Hedges g = 0.68; P < .001; k = 4), bulimia nervosa (Hedges g = 0.41; P = .001; k = 4), and binge-eating disorder (Hedges g = 0.34; P = .001; k = 7).
- “Anorexia nervosa exhibited the opposite pattern.”
- “Modest evidence of publication bias was indicated…”
A few thoughts:
- This is an important study.
- So do all patients with mental illness have greater delayed discounting than controls? The authors are careful in their wording: “The findings suggest that discounting is not universally increased in all psychiatric disorders but is more appropriately conceptualized as falling on a continuum.” I would add that those with anorexia nervosa didn’t fit the pattern.
- Meta-analyses are studies of studies, offering us a new look at existing data. This paper looks robust, and covers 43 studies. But, again, the total isn’t so great. Some of the individual papers have small samples (like the Engelmann et al. paper on depression, which drew on fewer than a dozen people with depression, albeit as a case control study). Still, a quick glance at the forest plots offers a clear pattern for all disorders spare anorexia nervosa (the squares are on the right side of the line consistently).
- Why would there be greater delayed discounting found across such different disorders? Is there a tie to a universal underlying mechanism (involving the limbic system or a neurotransmitter, like dopamine)? Is the explanation simply more concrete: that people with mental illness feel less well, making it harder to focus on the future.
- We can wonder about future research. Are there clusters of symptoms with major depressive disorder, for example, that would tie more to delayed discounting than other clusters of symptoms?
- There are clear clinical implications. Think communication. We often speak to patients about benefits in the future (take a pill a day, and you may feel better in 6-8 weeks) that may be more challenging for our patients to appreciate (as opposed to suggesting that the medications will improve sleep and energy over the coming days, and mood over the coming weeks). Think therapy. Should psychotherapies emphasize future thinking? Think family support. Families often look for ways to help their loved ones; can reminders about future planning be part of that?
- Are there behavioural economic implications? If the ultimate idea is to nudge people to good choices (staying on medications long term, rather than going off their medications, for example), the results suggest unique challenges for those with mental illness.
- I’ll congratulate the authors on adding nicely to a growing literature – albeit with a heavy title.
- For more on mental health care and behavioural economics, see these past Readings: https://davidgratzer.com/reading-of-the-week/reading-of-the-week-smoking-cessation-incentives-the-nejm-paper/ and https://davidgratzer.com/reading-of-the-week/reading-of-the-week-better-pay-better-service-the-cmaj-paper-on-pay-for-performance-in-psychiatry-also-a-fathers-memory/
“Lithium: the gripping history of a psychiatric success story: The treatment for bipolar disorder was discovered through an unlikely route.”
Douwe Draaisma
Nature, 26 August 2019
https://www.nature.com/articles/d41586-019-02480-0
Some 70 years ago, John Cade, an Australian psychiatrist, discovered a medication for bipolar disorder that helped many patients to regain stability swiftly. Lithium is now the standard treatment for the condition, and one of the most consistently effective medicines in psychiatry. But its rise was riddled with obstacles. The intertwined story of Cade and his momentous finding is told in Lithium, a compelling book by US psychiatrist Walter Brown.
Bipolar disorder, labelled manic-depressive illness until 1980, affects around 1 in 100 people globally. Without treatment, it can become a relentless cycle of emotional highs and lows. Suicide rates for untreated people are 10–20 times those in the general population. Fortunately, lithium carbonate – derived from the light, silvery metal lithium – can reduce that figure tenfold.
Brown’s telling of Cade’s eventful life covers much of the same ground as Finding Sanity (2016), a rather hagiographic biography by Greg de Moore and Ann Westmore. What Brown does superbly well is to show that Cade made his discovery without access to advances in technology or to modern facilities – and almost despite them. His finding was the happy result of being forced to work with the simplest of means.
 Douwe Draaisma
Douwe Draaisma
So opens a book review just published in Nature by Draaisma.
The book (and this book review) focuses on John Cade, the Australian psychiatrist, who injected patients’ urine into guinea pigs.
Cade found that lithium carbonate – which had been used to treat conditions such as gout since the nineteenth century – reduced the toxicity of patients’ urine. Cade also noticed that a large dose of the medication tended to calm the guinea pigs. He could turn them on their backs, and the normally restive rodents would gaze placidly back at him. He wondered whether lithium could have the same tranquillizing effect on his patients. After trying it out on himself to establish a safe dose, Cade began treating ten people with mania. In September 1949, he reported fast and dramatic improvements in all of them in the Medical Journal of Australia…
Draaisma notes that reads are “left with a sense of paradox.”
The drug that set off the ‘psychopharmacological revolution’ of the 1950s, with antipsychotics and antidepressants arriving in its wake, is in many ways a stunning success. Yet it was developed in a ramshackle pantry, and the bottled urine samples were stored in the Cade family refrigerator. Moreover, in retrospect, the discovery of lithium seems in part related to an erroneous interpretation on Cade’s part. The ‘tranquillized’ guinea pigs were probably showing the first symptoms of lithium poisoning: lethargy is still a warning sign of an overdose. And the step from guinea pigs to humans was a “conceptual leap”, as Brown kindly puts it – hardly a deduction from sound theory. It is unlikely that a modern researcher would get permission for experiments such as Cade’s.
A few thoughts:
- This is a good book review.
- The story reads well, and reminds us of the rough beginnings of psychopharmacological era.
- Dr. Cade’s original paper can be found here: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2560740/pdf/10885180.pdf.
- This month marks the fifth anniversary of the Reading of the Week in its current form. The first selection of that first Reading was on lithium. We have come full circle.
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments