From the Editor
Does pay for performance work for psychiatry?
This week’s first selection is a paper just published by CMAJ that considers that question. Drawing on Ontario data, the authors looked at practice patterns when financial incentives were introduced for psychiatrists to take care of patients after discharge and after suicide attempts. Spoiler alert: they didn’t work.
 Paying for Performance – Getting Performance?
Paying for Performance – Getting Performance?
In this Reading, we consider the paper and the larger debate.
We also consider a short, moving essay by radio host Charles Adler on the memory of his father – and his father’s memory. The award-winning broadcaster describes his father and his Alzheimer.
DG
Bonuses and Practice
“Payment incentives for community-based psychiatric care in Ontario, Canada”
David Rudoler, Claire de Oliveira, Joyce Cheng and Paul Kurdyak
CMAJ, 11 December 2017
http://www.cmaj.ca/content/189/49/E1509
Pay for performance has been employed by many jurisdictions to improve the delivery of evidence-based care, to expand access and to improve health outcomes. In Canada, some provinces have implemented pay-for-performance incentives, particularly for primary care physicians, despite the equivocal and limited nature of the evidence supporting them. In September 2011, the government of Ontario introduced bonus payments to encourage psychiatrists to provide rapid access to patients within 30 days of discharge after a psychiatric hospital admission and for 6 months after a suicide attempt. These are both high-risk periods for adverse events, and there is evidence that access to timely follow-up care may reduce the risk. By encouraging the delivery of follow-up care, the objective of these incentives was to help reduce the risk of deterioration, early readmission to hospital and possibly further suicide attempts. Implementation of these incentives followed similar attempts by provincial governments to improve the supply of services to high-risk patients in primary care settings. In particular, the government of Ontario has introduced incentives to encourage primary care physicians to roster patients with severe mental illness. In British Columbia, incentives have been implemented to encourage primary care physicians to create mental health care plans in collaboration with patients with a diagnosed mental illness.
In this study, we investigated whether psychiatrists changed their practice patterns in response to the September 2011 incentives, and whether patients at high risk had better access to psychiatrists. Our research questions were as follows: What is the effect of financial incentives on psychiatrist supply of community-based mental health and addiction care after discharge from hospital or after a suicide attempt? Can financial incentives increase access to community-based psychiatric care for patients after discharge or after a suicide attempt?
 David Rudoler
David Rudoler
So opens a new paper by Rudoler et al.
Here’s what they did:
- The authors drew from Ontario Ministry of Health data which included “information on physician and practice characteristics, physician claims, patient characteristics, admissions to designated psychiatric hospital beds, emergency department visits and suicide attempts.”
- The study period was September 2009 to August 2014.
- Exclusion criteria included patients under 16 and those not eligible for public insurance.
- They focused on three payment incentives: billing codes K187 (a 15% premium on some outpatient care within 30 days after a psychiatric discharge), K188 (a 15% premium for some services within 180 days of a suicide attempt), K189 (an annual $200 fee for each patient followed within 4 weeks of psychiatric discharge for 6 months).
- Two outcomes were considered: at the psychiatrist level, if there was a change in the rate of incentive-eligible service provided after hospital discharge or after a suicide attempt; at the patient level, if there was a change in the likelihood receiving the incentive-eligible service.
- Statistical analyses were done to consider practice and patient experiences before and after the incentives were introduced.
Here’s what they found:
- The sample included 1,921 psychiatrists who were followed for 60 months, and included 304,574 patients who had been discharged after a psychiatric hospital admission and 78,375 patients with a previous suicide attempt.
- “We found that the average quantity of monthly visits per psychiatrist provided after discharge decreased after the introduction of the payment incentives (from 1.50 to 1.43), as did the quantity of monthly visits provided after a suicide attempt (from 1.35 to 1.23)”
- “The results of our interrupted time-series analysis suggest that there was no immediate effect of the incentives on the quantity of visits supplied to patients after hospital discharge (mean change in visits per month per psychiatrist 0.0099 to 0.1206) or after a suicide attempt (mean change −0.0910 to 0.0026).”
- “The findings from our patient-level analysis suggest that the likelihood of receiving an eligible visit after hospital discharge or after a suicide attempt remained static over the study period. Implementation of the incentives had no immediate effect on the probability of a patient seeing a psychiatrist 30 days after discharge (change in level −0.0079 to 0.0061; change in trend 0.0007 to 0.0016) or 180 days after a suicide attempt (change in level 0.0074 to 0.0366; change in trend 0.0006 to 0.0022).” See figure below.
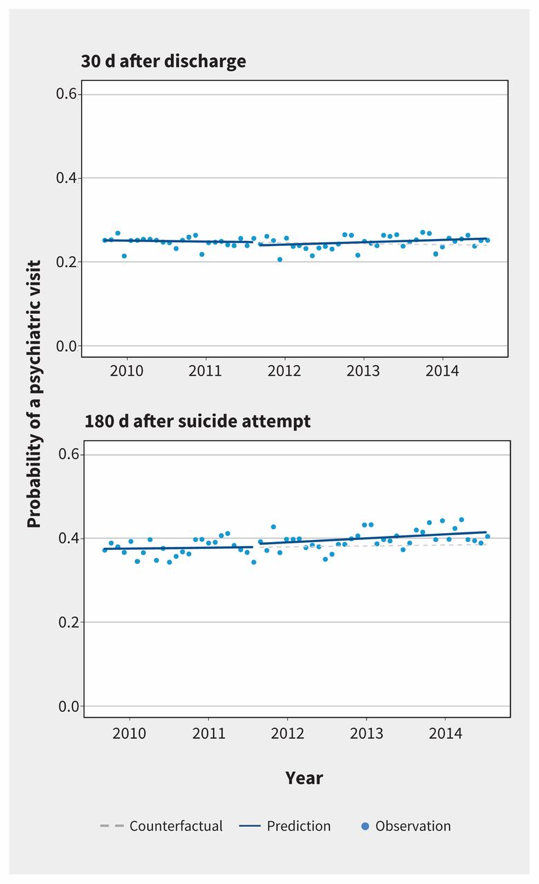
The 3 incentives implemented in Ontario did not have a meaningful effect on psychiatrist behaviour or on the likelihood that patients would receive psychiatric care after discharge from hospital or after a suicide attempt. The rates of follow-up care and the quantity of follow-up services provided remained static over the study period.
A few thoughts:
- This is a good paper.
- With regard to incentives, the study showed that there was no “meaningful effect.” Why? The authors considered this, and mulled several explanations. They considered, for example, that the incentives themselves were too small. “Using the average fee for eligible services, the incentive payment per eligible service was about $30, which may not have been large enough to alter psychiatrist behaviour or to encourage psychiatrists to incorporate the incentive codes into their usual billing routines.”
- In terms of pay for performance, the surprise here is that anyone would be surprised. Pay for performance makes sense in theory – doesn’t everyone respond to incentives? – but it doesn’t seem to actually influence physician behaviour in the real world. As this study showed, in the Ontario psychiatry context, the incentives didn’t do much. Writing in The New York Times, Dr. Aaron E. Carroll reviews the larger literature, finding mixed results at best. For instance, an ambitious UK program to pay family doctors robust bonuses for good management of chronic illness “made no difference at all in physician practice or patient outcomes…” You can find the article here: https://www.nytimes.com/2014/07/29/upshot/the-problem-with-pay-for-performance-in-medicine.html?_r=0.
- If small incentives don’t make a difference, what would? The Globe and Mail considered this with a longer article written by reporter Erin Anderssen. Study co-author Paul Kurdyak suggests we look at other countries.
Although specialists are only one part of an overwhelmed mental-health system, Dr. Kurdyak’s work points to the need for steps already taken in countries such as Britain and Australia, where psychiatrists serve almost exclusively as consultants, provide continuing care for the most severe mental illnesses, and are paid significantly less to provide talk therapy.
In the United States, Dr. Kurdyak says, some private health insurers withhold payments to hospitals for treating mental-health patients until they have been seen by a psychiatrist after their discharge – a recognition, he points out, that follow-up care improves recovery rates and saves the system money, particularly in cases of relapse. (Some of the patients in the study may be seen by their family physicians, says Dr. Kurdyak, but the severity and complexity of their cases merit more expert care.)
- Needless to say, the study and The Globe article have sparked discussion, including letters to the editor. Gary Chaimowitz and Desi Brownstone of the Coalition of Ontario Psychiatrists write:
Psychiatrists, like many health-care professionals, need to evolve the way they work. But studies demonstrate that patients benefit from the specialized assessments provided by psychiatrists, and that long-term treatment plans help those with severe mental illness and most at risk of suicide and other destructive behaviour.
They call for more residency spots for psychiatry and a team-based approach.
You can find the letter here:
Fathers and Sons
“In memory of Mike Adler, who survived the Holocaust but couldn’t escape Alzheimer’s”
Charles Adler
Globalnews.ca, 18 December 2017
It’s 2 o’clock in the morning and sleep eludes me. It’s Dec. 18, three days away from the third anniversary of the death of Mike Adler, the man who gave me life, rescued my life and gave my life meaning.
Papa died on the fifth day of Hanukkah, a holiday he could no longer celebrate but this time, not because he was hiding from Nazis in his early 20s.
Now, in his early 90s, he couldn’t hide from Alzheimer’s. The disease that made him forget who his kids were also made him forget his heritage.
So it falls to the dutiful first-born to tell you a little about that.
 Charles Adler
Charles Adler
So opens a new blog by broadcaster Charles Adler. The piece is short and deeply moving. It doesn’t require much of a summary here.
Adler talks about his father’s survival in dark times – his father was an Orthodox Jew who served in his country’s army. Facing deportation to a concentration camp, he fled, hiding in neighbouring Romania, until the Soviet army arrived.
To Hungary, he was too Jewish. To the Soviets, he was too Hungarian. He was put on a train to Siberia where he would spend three years doing slave labour. He survived and when he returned to the Hungarian village where he grew up two years after the war had officially ended, he was told that his parents and baby sister and little brother were murdered.
Adler then discusses his father’s dementia.
As sleep eludes me, my mind can’t get past the cruelty that is visited on the innocent. Here’s a man who values his memory more than anything because of its living link to the innocents who were herded into cattle cars, worked to death and then herded into gas chambers. And while all he can do is cling to his memory, that precious memory is looted by this serial thief: Alzheimer’s.
Adler notes that his father had backpacked him out of the “fires of communism” when he was a child. “Will always think he would have done the same for me in a wheelchair.”
A final thought: this is a beautiful and moving essay.
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments