From the Editor
There are more COVID-19 cases in the community – and in our hospitals and ICUs. What does it mean for mental health?
This week, we have three selections.
In the first, published in JAMA, Dr. Naomi M. Simon (of the NYU Grossman School of Medicine) and her co-authors write about the pandemic and the implications for mental health. They argue that there will be a second wave of mental health problems. “The magnitude of this second wave is likely to overwhelm the already frayed mental health system, leading to access problems, particularly for the most vulnerable persons.” Are they right – and what’s to be done?

In the second selection, we look at a research letter from The Canadian Journal of Psychiatry. Paula Conforti (of the University of Toronto) and her co-authors consider a CBT intervention for school-age children to reduce suicidality and increase wellbeing. There’s a twist in the plot: the intervention is based on a Harry Potter novel. “This study found that a teacher-delivered, literature-based CBT skills curriculum was feasible and associated with reduced suicidality (ideation and behavior) in middle school-aged youth.”
Finally, in our third selection, we consider an essay by Andrea Bennett. In this Walrus essay, the writer discusses the possible link between bipolar and creativity. The essay is deeply personal. “I don’t dream about not being bipolar, because I don’t know where my self ends and where the illness begins – and if there is even really a difference.”
DG
Selection 1: “Mental Health Disorders Related to COVID-19–Related Deaths”
Naomi M. Simon, Glenn N. Saxe, Charles R. Marmar
JAMA, 12 October 2020 Online First

Since February 2020, the coronavirus disease 2019 (COVID-19) pandemic has led to at least 200 000 deaths in the US and 1 million deaths worldwide. These numbers probably underestimate COVID-19 deaths by 50%, with excess cardiovascular, metabolic, and dementia-related deaths likely misclassified COVID-19 deaths. In this issue of JAMA, Woolf and colleagues update their previous estimate, suggesting that the number of excess deaths between February and August 2020 attributable to COVID-19 is estimated to be about 225 000.
This devastating pandemic has affected nearly every aspect of daily life. While nations struggle to manage the initial waves of the death and disruption associated with the pandemic, accumulating evidence indicates another ‘second wave’ is building: rising rates of mental health and substance use disorders. This imminent mental health surge will bring further challenges for individuals, families, and communities including increased deaths from suicide and drug overdoses. As with the first COVID-19 wave, the mental health wave will disproportionately affect Black and Hispanic individuals, older adults, lower socioeconomic groups of all races and ethnicities, and health care workers.
So begins a paper by Simon et al.
There is the loss of life, but the authors also note the larger toll of the pandemic:
“The necessary social distancing and quarantine measures implemented as mitigation strategies have significantly amplified emotional turmoil by substantially changing the social fabric by which individuals, families, communities, and nations cope with tragedy. The effect is multidimensional disruption of employment, finances, education, health care, food security, transportation, recreation, cultural and religious practices, and the ability of personal support networks and communities to come together and grieve.”
They note survey data:
- “A June 2020 survey from the Centers for Disease Control and Prevention of 5412 US adults found that 40.9% of respondents reported ‘at least one adverse mental or behavioral health condition,’ including depression, anxiety, posttraumatic stress, and substance abuse, with rates that were 3 to 4 times the rates 1 year earlier.”
- “Remarkably, 10.7% of respondents reported seriously considering suicide in the last 30 days.”
“Of central concern is the transformation of normal grief and distress into prolonged grief and major depressive disorder and symptoms of posttraumatic stress disorder. Prolonged grief disorder is characterized by at least 6 months of intense longing, preoccupation, or both with the deceased, emotional pain, loneliness, difficulty reengaging in life, avoidance, feeling life is meaningless, and increased suicide risk.”
They propose:
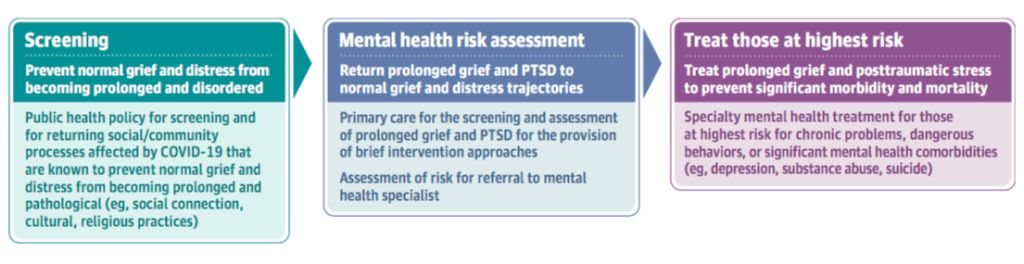
They focus on death and bereavement, advocating “a public health/community strategy is critical to protect the health care system from becoming overwhelmed.” This would involve caregivers and clinicians working together when a death occurs, particularly if the bereaved includes a child. They suggest the use of scales: “Primary care clinicians can use validated screening tools, such as the PTSD Checklist for posttraumatic stress disorder symptoms, the Patient Health Questionnaire 9 for depression symptoms, and the Prolonged Grief 12 questionnaire for prolonged grief symptoms, to proactively identify family members or friends of the deceased person who are at highest risk of developing mental health conditions.”
They also note the risk to essential workers:
“Of particular concern are psychological risks for health care workers and other essential workers who are providing care for patients with COVID-19. Health care workers must make challenging decisions such as how to distribute limited resources that may directly affect patient survival, may experience concerns about acquiring infection with severe acute respiratory syndrome coronavirus 2, and may experience anxiety, insomnia, and symptoms of traumatic stress, as well as moral injury, guilt, and shame.”
A few thoughts:
- This is an important paper.
- This Viewpoint paper has been published along with several others in JAMA, all considering COVID; authors have included public health experts, former presidential advisors, and a former US cabinet secretary. It’s nice to see a paper weighing mental health care included in the collection.
- The focus on chronic bereavement is interesting.
- CAMH, working with Delvinia (a tech company), has done several surveys looking at mood and anxiety symptoms over the course of the pandemic. To summarize much data in a single sentence: mood and anxiety symptoms have increased, as has drinking. Remember, though, that symptoms shouldn’t be confused with disorders. The point being that many will be stressed in difficult times, but they have the resilience to get through it. Returning back to the Simon et al. paper, they argue that some people are at greater risk, and screening and interventions should focus on groups with greater vulnerability, such as those who are bereaved and essential workers. This is an important point, and one made in other journals, including an excellent editorial in The Canadian Journal of Psychiatry by Vigo et al.
The full JAMA paper can be found here:
https://jamanetwork.com/journals/jama/fullarticle/2771763
Selection 2: “The Feasibility of a Harry Potter–based Cognitive Behavioural Therapy Skills Curriculum on Suicidality and Well-being in Middle Schoolers”
Paula Conforti, Rabia Zaheer, Benjamin I. Goldstein, et al.
The Canadian Journal of Psychiatry, November 2020
![]()
Suicide prevention in youth, for whom suicide is the second leading cause of death, is a public health imperative. Bolstering coping strategies through universal school-based interventions offers potential primary prevention of risk of self-harm and suicide in youth. While numerous suicide prevention interventions have been developed and implemented, effectiveness research remains scant, and the interventions are generally costly to implement, limiting ‘real-world’ application. The primary focus on imparting knowledge about suicide can be counterproductive, whereas stories of resilience and coping may impart protection (termed the Papageno effect) and mitigate the risks of focusing on suicide. Our group previously published data regarding a unique resiliency curriculum imparting cognitive behavioural therapy (CBT) skills to youth through the 3rd book in the Harry Potter series. During the curriculum, youth learn to cope with distress alongside the protagonist and to recognize that the novel is an allegory for the author’s own coping efforts to overcome depression. This prospective, pre–post, single arm intervention cohort feasibility study is the first to rigorously evaluate for effects on suicidality, anxiety, depression, and well-being in middle school-aged youth.
So begins a research letter by Conforti et al.
Here’s what they did:
- Eight English teachers were recruited from eastern Ontario.
- They taught the curriculum to grade seven and eight students.
- “The intervention was a novel study curriculum delivered over 3 months in January to April of 2019. Students read Harry Potter and the Prisoner of Azkaban and were taught CBT skills.”
- Students completed two questionnaires pre and post-intervention: the Life Problems Inventory (LPI) and the Revised Children’s Anxiety and Depression Scale (RCADS).
Here’s what they found:
- A total of 176 students received the informed consent package with 83 (47%) consenting to enrollment into the study.
- “Of these, 78 (94%), including 50 girls and 28 boys, had both pre- and post-measures and comprised the group used for data analysis.”
- “Suicidality scores improved by 44% following the curriculum with significant reductions for each of the four suicide questions. LPI scores also decreased by 11% overall with no significant change in RCADS scores…”
A few thoughts:
- This is a fun research letter based on a clever project.
- It’s also a thoughtful and creative project. Why not provide CBT skills to schoolchildren? In North America, short, focused psychotherapies are used to treat mental illness. There is evidence that they can have a preventive effect – and are used in places like Australia for that purpose.
- There is much to like here, but it’s not definitive like the results of a Quidditch championship; there was no control group.
- Having read through five of the Potter books with a young fan, I endorse the choice of Harry Potter and the Prisoner of Azkaban. Could a follow-up study draw from Harry Potter and the Order of the Phoenix? (Asking for a young fan.)
The research letter can be found here:
https://journals.sagepub.com/doi/full/10.1177/0706743720944046
Selection 3: “On Being Bipolar”
Andrea Bennett
The Walrus, 24 September 2020
![]()
Sometime in my mid-to-late twenties, less than a decade after I’d been diagnosed bipolar II, I participated in a study that sought to glean insights from ‘high-functioning’ bipolar people – presumably to figure out why we were high functioning and if anything we had to share could help others become high functioning too.
“The study took place in a little room in a low-slung building that seemed like it had been built in the seventies. The woman who administered the study was a grad student, maybe a bit younger than me. She proceeded to ask me questions about my diagnosis and mental health history. When she got to the part of the survey about hallucinations, she seemed apologetic, ready to skip it – bipolar people can but don’t always experience hallucinations and/or psychosis, and it’s less common with bipolar II than with bipolar I. ‘Oh,’ I said, ‘we will need to go through those.’
So begins an essay by Bennett.
The author bluntly describes the illness experience:
“The period of time in which I was hallucinating, I was also living in circumstances that the woman who was interviewing me probably would have found appalling. In the winter, my then partner and I wore toques and hoodies to bed because it was too cold not to; at the very end of my bachelor’s degree, which coincided with the peak of one of his binges, I woke up to write my final exam and had to walk over him, as he was passed out on the floor and surrounded by broken glass, to get to the coffee maker. I was taking lithium. I saw birds in the corners of our rooms – one owl, in particular, recurred. I heard a low, echoing voice. I knew these things were hallucinations, and for the time I experienced them, I lived with them just like I lived with my then boyfriend’s alcoholism and the broken glass on the floor.”
That experience runs in contrast to the depiction in books and movies. Bennett argues that bipolar has been romanticized in popular culture.
“Bipolar disorder is depicted as a font of creativity, fun, and terrible choices. Virginia Woolf, Vincent van Gogh, Stephen Fry, Carrie Fisher, Charlie Sheen, Britney Spears, Chris Brown, Catherine Zeta-Jones, Lou Reed, Kim Novak, Edvard Munch, Marilyn Monroe: if you’re famous and bipolar, your name will begin to grace googleable lists, many devoid of any kind of context. You can be known for succeeding despite your diagnosis or you can be known for the train wreck you make of your life and career. The only way you can stake a claim on your own story is to tell it yourself, like Fry did.”
This assumption leads to conclusion about the illness experience itself. “The end result is that the story of being bipolar – an illness with ups and downs, which offers a narrative more easily than illnesses without – is one where, often, the manic protagonist must wrestle his euphoria to the ground for the sake of his better sanity. When you are manic, the understanding is that you enjoy your mania.”
Bennett writes: “Adjacent to the list of famous people with bipolar disorder that I can recite if asked is another list, a list of nonfamous people, friends and acquaintances. I won’t list them – they’re not famous, and their stories are not mine to tell. Two of them died by overdose, one accidentally and one not as accidentally. Both were people who maybe found it easier to care deeply about others than about themselves.”
A few thoughts:
- This is a good essay.
- Like other personal writing, this piece can be tough to read at points – not because of the prose itself, but because the rawness of the writing. (I made a similar comment about Dr. Horton’s essay last week.)
- Is bipolar disorder associated with greater creativity? Some have made that argument, including Kay Redfield Jamison in her classic book Touched with Fire. (Jamison, for the record, has bipolar disorder.)
- Still, Bennett makes a strong argument that we shouldn’t romanticize mental illness.
The full Walrus essay can be found here:
https://thewalrus.ca/on-being-bipolar/
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments