From the Editor
How to treat depression? How do we approach suicide? Who is the greatest Raptor of all time?
This week, we consider three pieces.
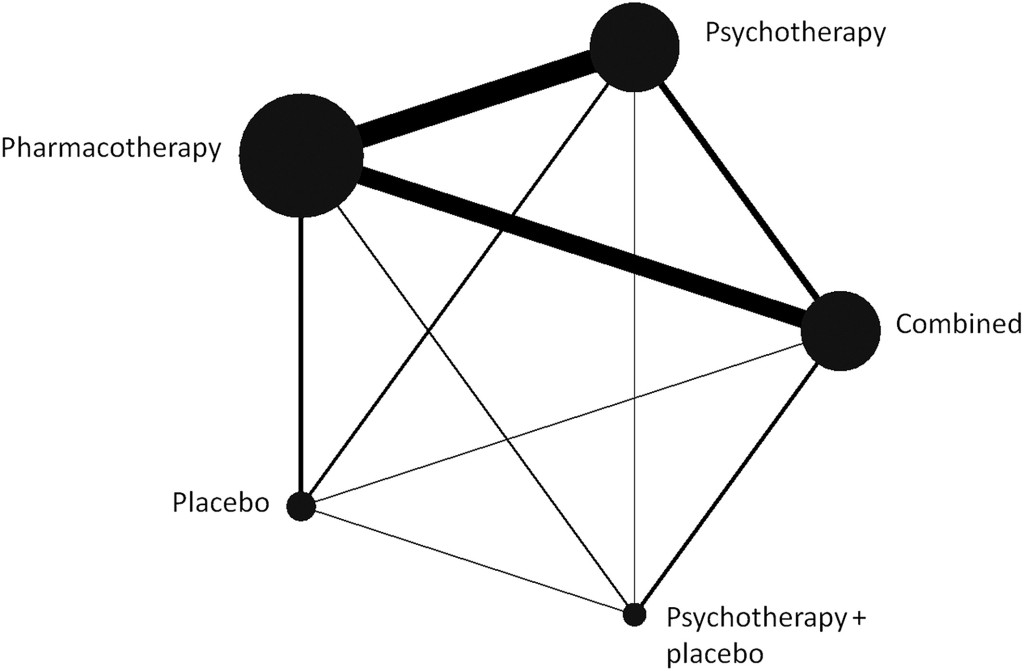
In the first selection, Pim Cuijpers (Vrije Universiteit Amsterdam) and his co-authors do a network meta-analysis of depression treatment, weighing psychotherapy, pharmacotherapy, and the combination of the two. They find: “combined treatment is more effective than psychotherapy or pharmacotherapy alone in the short‐term treatment of moderate depression, and there are no significant differences between psychotherapy and pharmacotherapy.”
In a short New England Journal of Medicine paper, Drs. Seena Fazel (Oxford University) and Bo Runeson (Karolinska Institutet) review a topic of relevance to all clinicians: suicide. “Management of suicidality calls for a comprehensive approach to assessment and treatment.”
 Yes, we talk about basketball this week
Yes, we talk about basketball this week
Finally, in the third selection, the University of Toronto’s Dr. Mark Sinyor writes about basketball and his favourite Raptor – and, yes, stigma.
DG
Selection 1: “A network meta‐analysis of the effects of psychotherapies, pharmacotherapies and their combination in the treatment of adult depression”
Pim Cuijpers, Hisashi Noma, Eirini Karyotaki, Christiaan H. Vinkers, Andrea Cipriani, Toshi A. Furukawa
World Psychiatry, February 2020
![]()
No network meta‐analysis has examined the relative effects of psychotherapies, pharmacotherapies and their combination in the treatment of adult depression, while this is a very important clinical issue. We conducted systematic searches in bibliographical databases to identify randomized trials in which a psychotherapy and a pharmacotherapy for the acute or long‐term treatment of depression were compared with each other, or in which the combination of a psychotherapy and a pharmacotherapy was compared with either one alone.
So begins the abstract for a new paper by Cuijpers et al.
Here’s what they did:
- They did a search of major databases (including Pubmed) using keywords indicative of depression and psychotherapies, with a filter for RCT.
- “We included studies in which a psychotherapy and a pharmacological treatment for depression were directly compared with each other, and studies in which the combination of a psychotherapy and a pharmacological treatment was compared with either one alone.”
- Only patients with acute depressive disorders were included; comorbid mental or somatic disorders were not excluded.
- “Treatment response, defined as a 50% reduction in depressive symptomatology according to a standardized rating scale, was chosen as the primary outcome.”
- In terms of the meta-analysis: “We conducted pairwise meta‐analyses for all comparisons, using a random effects pooling model… The comparative effectiveness was evaluated using the network meta‐analysis methodology.”
Here’s what they found:
- A total of 101 studies met inclusion criteria, involving 11,910 participants combined.
- “CBT was the most commonly used psychotherapy (48 trials); an individual format was used in 81 psychotherapy studies; 45 trials met all three quality criteria. SSRIs were the most frequently used medications; pharmacotherapy was judged adequate in 67 trials.”
- Meta-analysis: “Combined treatment was more effective than both psychotherapy alone (RR=1.25) and pharmacotherapy alone (RR=1.27). The difference between psychotherapy alone and pharmacotherapy alone was not significant…”
- Network: See the figure below for the plot rate. “Combined treatment was superior to either psychotherapy alone or pharmacotherapy alone in terms of response (RR=1.27 and RR=1.25, respectively), remission (RR=1.22 and RR=1.23)…” More – “Acceptability was significantly better for combined treatment compared with pharmacotherapy (RR=1.23), as well as for psychotherapy compared with pharmacotherapy (RR=1.17).” (!)
This is a good and interesting study. But it should be pointed out that network meta-analyses aren’t without controversy. Still, there is much to like here, including the fact that the co-authors include Pim Cuijpers and Andrea Cipriani, and the paper was published in the journal with the highest impact factor in psychiatry.
Two quick observations.
First, with this exhaustive approach pooling together over a hundred papers, the authors come to the same conclusion as the CANMAT guideline authors: depression treatment should involve more than just medications. Second, there are strong implications for our Canadian patients who rarely have the opportunity to receive more than medication management (Puyat et al. found that just 13% of British Columbians with depression receive counseling or therapy).
https://onlinelibrary.wiley.com/doi/full/10.1002/wps.20701
Selection 2: “Suicide”
Seena Fazel and Bo Runeson
The New England Journal of Medicine, 16 January 2020

Throughout the world, approximately 800,000 people die by suicide every year, accounting for 1.5% of all deaths. Suicide is the 10th leading cause of death in North America and the foremost cause of death worldwide among persons 15 to 24 years of age.
So begins a short, concise, and thoughtful paper on suicide.
On Epidemiology
“The World Health Organization (WHO) estimated that the 2016 suicide rate was 10.6 suicides per 100,000 persons…”
“80% of suicides occurring in low- and middle-income countries…”
On Risk Factors
“Individual factors, particularly psychiatric disorders,have the strongest effect on suicide rates in life-course models. Depression, bipolar disorder, schizophrenia-spectrum disorders, substance use disorders, epilepsy, and traumatic brain injury each increases the odds of completed suicide by a factor of more than 3. Other predisposing factors include a previous suicide attempt, childhood sexual abuse, a family history of suicidal behavior, and loss of a parent to suicide in early childhood.”
On Genetics
“A family history of suicide is a risk factor for suicide,with some evidence suggesting that a mother’s suicidal behavior has a greater influence than a father’s suicidal behavior.”
On Assessing Risk
“These assessment tools may increase the clinical workload by requiring psychiatric assessment or hospitalization in cases of false positive risks of suicide. In the case of some of these tools, most of the patients who ultimately died by suicide were predicted to be at low risk. Nevertheless, structured tools can provide a baseline assessment during initial contact with health care providers, offer a checklist to identify risk factors, and lead to interventions for those persons who are predicted to be at high risk for suicide.”
They note that U.S. National Strategy for Suicide Prevention recommends the use of suicide prediction tools,as does the European Psychiatric Association. “Despite the putative advantages of such tools, current evidence to support their routine use in emergency departments and in primary care is weak.”
On Pharmacological Treatments
“The few randomized trials of such treatment have been underpowered to study suicide and have relied on proxy outcomes (e.g., suicidal ideas or depressive symptoms).”
The authors note that there is evidence for antipsychotics in those with schizophrenia, and lithium for patients with bipolar disorder.
On Psychological Treatments
A meta-analysis that included various psychological treatments showed that at the end of the treatment period, interventions that directly addressed suicidal thoughts and behaviors and provided strategies for coping with them had better outcomes than treatment for anxiety and depression, but these differences were diminished after 1 year.
The authors review the literature: there is evidence that CBT reduces suicidal thoughts; mindfulness improves mood stability; DBT “has reduced self-harm in 12 trials but with small effect sizes;” a study showed that Internet-administered self-help treatments may help (this result wasn’t replicated – and we can consider it early evidence).
Here are few thoughts on this excellent paper:
- Suicide is a problem across all nations, but the majority of suicides occur in the low and middle-income nations – showing again the incredible challenges faced by global psychiatry.
- The paper does an excellent job of summarizing the literature. It’s difficult not to feel the thinness of past research, however, in particular in areas around interventions, in part because of the challenges of understanding suicide, an act so catastrophic if rare.
- The paper doesn’t focus on practical tips for clinicians, but certainly points in the direction of more use of scales. (For the record, my colleague Dr. Juveria Zaheer suggests that we should be using PHQ-9s more frequently.)
https://www.nejm.org/doi/full/10.1056/NEJMra1902944
Selection 3: “DeMar DeRozan helped change the conversation about mental health”
Mark Sinyor
Toronto Star, 5 January 2020
![]()
On Jan. 12, the Raptors welcome the San Antonio Spurs and the greatest Raptor of all time back to the Scotiabank Arena. Apologies to Kawhi, who was dynamite during his pit stop in Toronto, and to Kyle, who is definitely in the conversation.
But DeMar DeRozan was the best Raptor for five of the team’s six-and-a-half year emergence into NBA relevance and he remains the GOAT. I suspect that a fair number of my fellow We The Northers will agree, but I have a different perspective than most.
He then draws on his own experience – and DeRozan’s.
I co-ordinate the outpatient mood disorders clinic at Sunnybrook Hospital and that makes me lucky enough to have a daily front row seat to witness people with mental illness finding ways to overcome incredible adversity. It’s true that the road for many is bumpy but so much more often than not, their stories are inspiring and in such contrast to the ‘if it bleeds it leads’ narratives that too often pervade the popular press and social media.
So I paid extra attention when, during the 2018 All-Star break, DeRozan posted ‘This depression get the best of me …’ in the middle of the night on Twitter.
He goes on to discuss the full weight of those comments:
“But it’s a constant battle because illnesses like depression make sufferers feel hopeless and many, especially men, still have the tragic impression that seeking help is weak or even shameful. So when DeRozan opened up, prompting other NBAers like Kevin Love and Channing Frye to do the same, he gave this city and his fans a gift that goes far beyond basketball.”
“His words have helped to change the conversation about mental illness. Their impact will be wider reaching and longer felt than any victory parade.”
This is a fun essay, but it’s also an important piece of public advocacy, taking our message to a general readership.
For the record, Dr. Sinyor makes good points – though I’m not sure if I’m fully persuaded about the greatest Raptor of all time…
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments