From the Editor
This time of year, many doctors take to social media to offer advice to young colleagues as they start their specialty training (#TipsForNewDocs). Generally, the tweets give solid suggestions on everything from the importance of mentorship to doing regular exercise. For those new grads beginning psychiatry training, I offer: read more, the field is evolving. Since I started my psychiatry residency 19 years ago this month, we have seen new antidepressants placed into the drug cabinets of our patients, mental-health apps populate their smart phones, and clinical guidelines enter our practices, helping us better manage their mental illness.
This week’s Reading focuses on cutting-edge care, and there is plenty to read.
In our first selection, we consider a new paper from The New England Journal of Medicine. Written by Dr. Jean Kim and four other FDA officials, the authors discuss esketamine for depression. “The drug represents an important addition to the treatment options for patients with treatment-resistant depression.”
 Esketamine: from club drug to depression care
Esketamine: from club drug to depression care
In our second selection, Dr. John Torous (of Harvard Medical School) and Rheeda Walker (of the University of Houston) consider digital psychiatry and suicide prevention, reviewing the field with cautious optimism. The paper opens with a single sentence that puts these efforts in perspective: “Because the rates of suicide attempts and deaths have recently increased to 50-year highs,new solutions are needed.”
And, in our third selection, we look at a not-so-new editorial from The American Journal of Insanity that calls for better treatment of the poor.
Enjoy.
DG
Selection 1: “Esketamine for Treatment-Resistant Depression — First FDA-Approved Antidepressant in a New Class”
Jean Kim, Tiffany Farchione, Andrew Potter, Qi Chen, Robert Temple
The New England Journal of Medicine, 4 July 2019

Treating major depressive disorder remains an important challenge worldwide. The disorder impairs productivity, social functioning, and overall health, reducing life expectancy and burdening health care systems. Although many treatments exist, at least a third of patients do not have a response after two or more trials of antidepressant drugs and are considered to have treatment-resistant depression.
The Food and Drug Administration (FDA) has approved only one drug for treatment-resistant depression: a fixed-dose combination of olanzapine and fluoxetine. Most antidepressants take several weeks to begin working.
So begins a New England Journal of Medicine perspective paper written by five FDA officials. They note that: “The FDA recently approved the S-enantiomer of ketamine, esketamine, a rapidly acting drug shown to be effective in patients with treatment-resistant depression. Ketamine, a noncompetitive antagonist of glutamate receptors of the N-methyl-d-aspartate (NMDA) type, was approved in 1970 as an anesthetic.”
They summarize the different clinical trials:
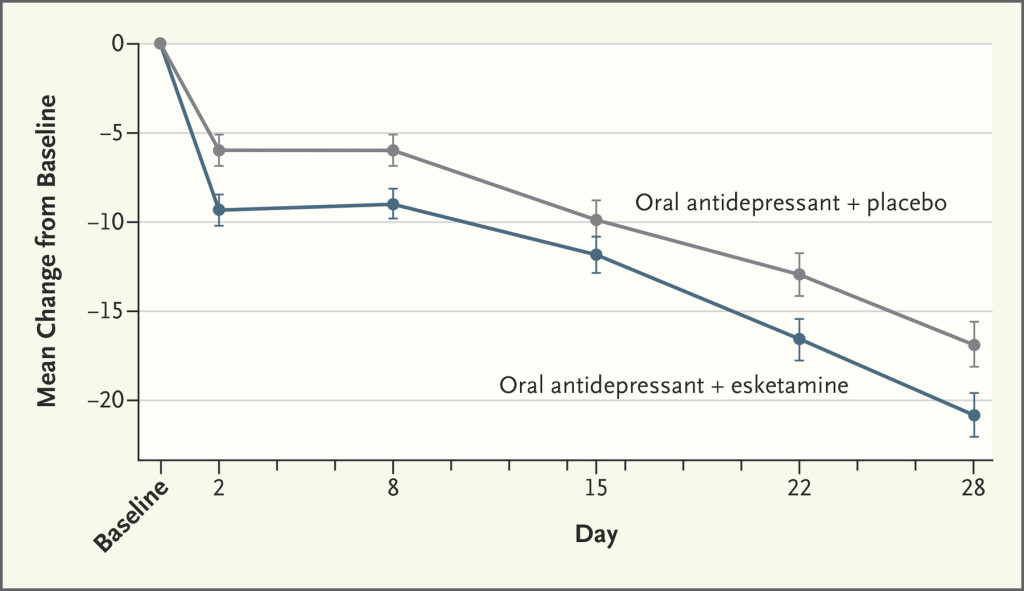
- Study 3002. Patients were assigned esketamine or placebo. With the former offering a statistically significant advantage at day 28. “Moreover, the treatment effect was apparent at day 2 (time of first assessment) – an unusually rapid onset…” See graph below.
- Study 3003. “The study provides important evidence that esketamine is effective beyond 1 month in patients who have an initial response.”
- Study 3001 and 3005 (a geriatric population). “Two short-term studies, Study 3001 and Study 3005, failed to demonstrate a statistically significant treatment effect.”
This paper outlines well the results from these studies. It’s interesting to note that the FDA took the potential of abuse seriously. Indeed, the FDA approved the drug with a Risk Evaluation and Mitigation Strategy “to mitigate the risk of serious adverse outcomes resulting from sedation, dissociation, and abuse and misuse, while providing access to this effective treatment for treatment-resistant depression.” Among the requirements: “esketamine will be dispensed and administered to patients only in a medically supervised health care setting…”
They conclude:
“Esketamine represents a novel treatment for a severe and life-threatening condition, and its rapid onset of effect is a key benefit. The studies provide evidence of clinically meaningful efficacy when esketamine is used in combination with a newly initiated oral antidepressant. With implementation of a REMS to ensure safe use and minimize abuse potential, the benefit–risk balance is favorable, and the drug represents an important addition to the treatment options for patients with treatment-resistant depression.” Among the requirements: esketamine be used “only in a medically supervised health care setting where they can be monitored for adverse reactions for at least 2 hours…”
Esketamine is very cutting edge. Past readings have the emerging literature (for the early evidence for acutely suicidal inpatients, see: http://davidgratzer.com/reading-of-the-week/reading-of-the-week-suicidal-get-a-postcard-the-new-jcp-paper-on-suicide-prevention-also-ketamine-inpatients/).
Time will tell whether this medication makes a mainstay of treatment for those with depression who failed much else, or if older treatments like ECT remain the gold standard.
#TipsForNewDocs: New isn’t necessarily better.
https://www.nejm.org/doi/full/10.1056/NEJMp1903305
Selection 2: “Leveraging Digital Health and Machine Learning Toward Reducing Suicide – From Panacea to Practical Tool”
John Torous and Rheeda Walker
JAMA Psychiatry, 10 July 2019 Online First

Because the rates of suicide attempts and deaths have recently increased to 50-year highs, new solutions are needed. The urgency to reverse this trend has brought attention to technology-based tools, such as text messaging, smartphone apps, smartphone sensors, electronic health records, and machine-learning algorithms, that can offer crucial data to improve the prognostication of suicide or immediate support for those at risk. This promise of real-time data from connected devices, large quantities of social-behavioral interactions from social media and internet, and longitudinal clinical trends from electronic health records, when paired with artificial intelligence to automatically identify risk, is often touted as a panacea.
But if the authors outline the potential, they are clear-eyed in their assessment of the present: “Yet, to date, this approach has found less clinical success than expected.”
They focus on three gaps in health care that contribute to suicide death.
A failure to proactively identify suicide risk. The authors write about “classic risk factors” but also note “overlooked risk factors” (like the diagnosis of cancer) and “dynamic risk factors” (e.g., sleep dysregulation). “[R]isk factors obtained from digital sources will likely be of maximal benefit when paired with algorithms that can contextualize that risk via dynamic models and translate population-level risk into personalized prognostications.”
Absent and inefficient safety planning. Follow-up phone calls and other brief interventions can be helpful, and the authors wonder about digital interventions. “While it is easy to image how elements of safety planning could be translated onto a web-based computer program, text-messaging platform, smartphone app, or even smartwatch feature and thus made even more accessible and scalable, it is important to note that the current evidence for available digital tools, such as smartphone apps, for suicide prevention is limited and with mixed results.”
Limited supportive contacts. They note that interventions like hand-written letters could change as they “are replaced with pixels on a screen.” They see a role for digital options, but not necessarily a sweeping one: “As an example, digital resources may be more effective for a father who has a history of major depressive disorder without a history of suicide attempt, has experienced a recent job loss, and is overwhelmed with the task of finding a new job to support his family, compared with that same father when he has been recently discharged from an inpatient psychiatric care unit after a suicide attempt. In the second scenario, the individual is at much higher risk for a suicide attempt and warrants a level of care that currently exceeds smartphone use alone.”
This paper is thoughtful, and doesn’t oversell. It concludes reasonably: “Technology is not the panacea of suicide prevention, but it is a crucial tool that the field must develop today to save lives tomorrow.”
#TipsForNewDocs: if suicide prevention was easy, they would have replaced us with computers by now.
https://jamanetwork.com/journals/jamapsychiatry/article-abstract/2737419
(On a side note, I had the opportunity to recently interview Dr. Torous on digital psychiatry, and the podcast can be found here: https://www.porticonetwork.ca/web/podcasts/quick-takes/digital-psychiatry.)
Selection 3: “Asylums Exclusively For The Incurable Insane”
The American Journal of Insanity, July 1844
Some benevolent individuals noticing the deplorable situations of the incurable insane, who are confined in poor-houses, and having seen the comfortable condition of deranged persons in well conducted Lunatic Asylums, have proposed that public Asylums should be built on a cheap plan, solely for those supposed to be incurable.
Establishments solely for the poor and incurable we believe would soon become objects of but little interest to any one, and in which neglect, abuse and all kinds of misrule would exist, and exist without detection.
This is an interesting paper, published in the first issue of The American Journal of Insanity (now The American Journal of Psychiatry). The authors caution against worse treatment of the poor; they also note the dangers of concluding that some are beyond hope.
The third in our series of three selections this week, an historic paper doesn’t seem particularly cutting edge. Yet the theme of equity and the call for better access for those with mental illness remain relevant, and perhaps still cutting edge.
#TipsForNewDocs: there is nothing new under the sun.
A quick word of congratulations to the editors of The American Journal of Psychiatry on their 175th anniversary. The first issue was published this month in 1844.
https://ajp.psychiatryonline.org/doi/10.1176/ajp.1.1.50
For those wanting to read more about cutting-edge care, the July issue of The Canadian Journal of Psychiatry runs an “in review” series on digital psychiatry, and opens with an editorial that weighs e-therapies, chatbots, and VR; that paper is informative (but I may be a bit biased). You can find it here: https://journals.sagepub.com/doi/metrics/10.1177/0706743719850057
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments