From the Editor
She presented to the emergency department with suicidal thoughts but no specific plan. She had been diagnosed with borderline personality disorder, and asked me a simple question: how can I do better?
In a new study published in The American Journal of Psychiatry, Beth S. Brodsky (of Columbia University) and her co-authors attempt to answer that question. 84 people with borderline personality disorder and past suicide attempts and/or self-harm behaviours were randomized and then offered either six months of therapy (DBT) or medications (SSRIs), and compared for the reduction of suicide attempts and self-harm. “DBT appears to work faster and perhaps more effectively in borderline personality disorder for suicide-related outcomes and for nonsuicidal self-injury compared with SSRIs plus clinical management.” We consider the study and its implications.

In the second selection from JAMA Psychiatry, Drs. Olga Terechin, Sofia E. Matta, and Joji Suzuki (all of Harvard University) propose that naltrexone be made available over the counter. Noting the deep problems of unhealthy alcohol use, they argue that greater availability of this medication would be important. “We believe that allowing OTC access to naltrexone would serve as a groundbreaking approach to addressing unhealthy alcohol use, particularly for individuals who are hesitant to seek help or live in areas where access to treatment is limited.”
And in the third selection, S. L. Harper (of the University of Alberta) and her co-authors look at climate change anxiety in Canada. Drawing on a survey with almost 2 500 participants, they analyzed prevalence and demographics in a Nature Mental Health paper. “Mild-to-moderate climate change anxiety in Canada is not uncommon… and certain demographic groups may require additional supports to manage and reduce the symptoms…”
DG
Selection 1: “Dialectical Behavior Therapy Versus Serotonin Reuptake Inhibitor Treatment for Suicidal Behavior in Borderline Personality Disorder: A Randomized Controlled Trial”
Beth S. Brodsky, Hanga Galfalvy, J. John Mann, et al.
The American Journal of Psychiatry, 5 November 2025 Online First

Individuals diagnosed with borderline personality disorder (BPD) have an elevated risk for suicidal behaviors and nonsuicidal self-injury (NSSI). Reasons include impulsiveness, emotional reactivity, and high comorbidity between BPD and major depressive disorder (MDD). Treating suicidality and NSSI in this population requires that clinicians determine which symptoms to target for prevention.
Psychosocial interventions reduce suicidal and NSSI behaviors in BPD. Eighteen months of mentalization-based therapy was found to be comparable in effectiveness to 18 months of structured clinical management. Similarly, 12 months of general psychiatric management, a less resource-intensive intervention than mentalization-based therapy or dialectical behavior therapy (DBT), was comparable in efficacy to 12 months of DBT. Most evidence indicates that 12 months of DBT is more efficacious than treatment as usual in preventing suicide attempts and NSSI. In some 6-month trials, DBT was found to reduce suicidal and NSSI behaviors, which may facilitate treatment retention and cost savings.
High rates of comorbid depression raise the question of the role of antidepressant medications in lowering risks for suicidal behavior and NSSI in BPD. Yet, there is no single recommended best practice for psychopharmacological prevention of suicide or NSSI in individuals with BPD with or without MDD… The outcomes examined in most randomized controlled trials (RCTs) of medication efficacy for BPD have examined outcomes for general BPD symptoms rather than suicidal or NSSI behaviors. Despite inconclusive evidence of efficacy, SSRIs are often employed for BPD and comorbid depression.
Here’s what they did:
- They conducted an RCT with people aged 18-55, comparing DBT and SSRIs + clinical management (SSRI/M).
- The inclusion criteria: a diagnosis of BPD; suicidal ideation within the past week; at least one episode of NSSI, suicide attempt, or suicide-related behaviour in the past 6 months, and another of these behaviours within the past year.
- Participants were randomly assigned to receive DBT or SSRI/M. “Allocation to the DBT treatment arm involved weekly individual DBT psychotherapy sessions, weekly skills group, and between-session skills phone coaching. Therapists attended a weekly peer consultation group.” “For those randomized to SSRI/M, fluoxetine was started at 20 mg/day, and the maximum dosage was set at 40 mg/day, because higher dosages are not more effective for treating depression…” Patients could be switched to citalopram and then paroxetine because of issues with tolerability or nonresponse.
- Statistical analyses included Poisson models to assess the numbers of suicide attempts and SREs.
Here’s what they found:
- 84 participants were randomized to the DBT and SSRI/M groups.
- Demographics and illness experience. The mean age was 29.3 years, and the sample was predominantly female (92%) and White (57%). 68% had comorbid MDD. 95% had past SREs and 71% had past histories of suicide attempts.
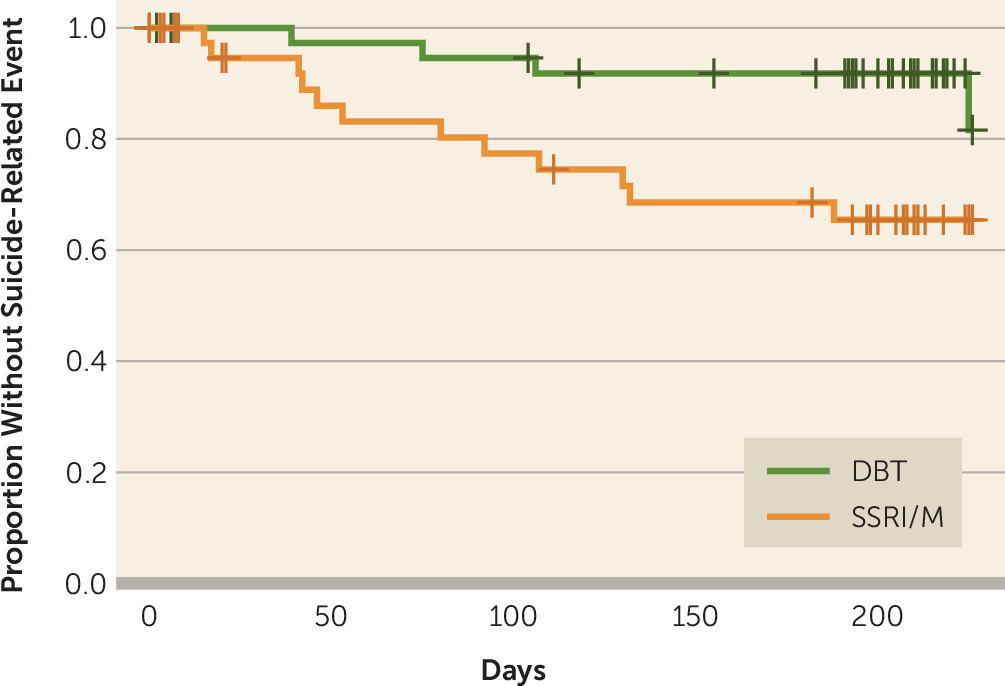
- Suicide-related events. Significantly fewer SREs occurred in the DBT arm compared with the SSRI/M arm during the 6-month treatment phase (four versus 12).
- Suicide attempts. The DBT arm had significantly fewer attempts than the SSRI/M arm (four versus nine).
- Analysis. Survival analysis indicated significantly lower risk for having any SRE in the DBT arm compared with the SSRI/M arm, but no difference in risk of suicide attempt.
- Self-harm. DBT participants had significantly lower NSSI counts than SSRI/M participants (about 30% less).
- Depression. After 6 months of treatment, the rate of major depressive disorder was significantly lower in the SSRI/M arm compared with the DBT arm (26% versus 3%).
A few thoughts:
1. This is a good study with a practical research question, published in a major journal. There is much to like here, including that it’s an RCT.
2. The main finding in a sentence: “DBT resulted in fewer SREs, suicide attempts, and NSSI episodes compared with SSRI/M treatment over a 6-month trial.”
3. Perspective: “There are no other published RCTs comparing these two treatments head-to-head for these outcomes in people with BPD.”
4. That said, are the results particularly surprising? Clinicians like you and me know that DBT can be effective, helping patients achieve better coping skills, something that can’t be done with just pills.
5. Of course, there are clear implications for mental health services. For too many patients, medications are accessible and DBT isn’t. That’s a comment on what’s easy to provide, rather than what’s actually evidenced for treatment. For the record, my ED patient had already spent several months on a wait list for psychotherapy.
6. Like all studies, there are limitations. The authors note several, including a lack of standardization in SSRI use.
The full American Journal of Psychiatry paper can be found here:
https://psychiatryonline.org/doi/10.1176/appi.ajp.20240298
Selection 2: “Over-the-Counter Naltrexone to Address Unhealthy Alcohol Use”
Olga Terechin, Sofia E. Matta, Joji Suzuki
JAMA Psychiatry, 5 November 2025 Online First

Unhealthy alcohol use is highly prevalent in the United States, with almost half of all regular consumers reporting binge drinking (≥5 drinks per occasion for men, ≥4 for women) and a quarter reporting heavy drinking (≥5 binges in the past month). Binge and heavy drinking are associated with numerous health effects ranging from acute, such as injuries and motor vehicle crashes, to chronic, such as liver disease and alcohol use disorder (AUD). AUD causes significant morbidity and mortality, with the prevalence among individuals aged 12 years and older now exceeding 10%…
Naltrexone, 1 of the 3 US Food and Drug Administration (FDA)–approved medications for AUD (MAUD), is an opioid antagonist that decreases the rewarding effects of alcohol, helping to reduce heavy drinking and alcohol cravings. Despite its safety and efficacy, naltrexone is underused; it is used by less than 2% of those with AUD. This underuse is driven by limited clinician awareness, persistent stigma surrounding AUD, and limited accessibility of treatment…
Given the growing public health impact of unhealthy alcohol use and the barriers to accessing MAUD, we advocate for making oral naltrexone available over the counter (OTC) without prescription.
So begins a paper by Drs. Terechin, Matta, and Suzuki.
“OTC naltrexone could be a safe and effective harm reduction tool for individuals with any degree of unhealthy alcohol use who would not seek or be able to access treatment otherwise.” They continue: “Many individuals in the early stages of AUD do not pursue treatment due to stigma and shame, leading many to enter treatment only after significant medical, interpersonal, or occupational consequences. We understand this proposal may initially appear radical, yet it aligns with prior public health strategies that have expanded access to evidence-based interventions.”
Is there any precedence for this? The authors point to nicotine. “A switch from prescription to OTC was successfully implemented with nicotine replacement therapy (NRT) in 1996, significantly expanding access during smoking cessation efforts. OTC naltrexone would align with the growing effort to provide low-threshold treatment for substance use disorders by allowing same-day access to medications, a harm-reduction approach, flexibility, and wide availability. While clinical indications differ, naloxone nasal spray – an opioid antagonist used for overdose reversal – was recently made available OTC, expanding access to a lifesaving harm-reduction intervention.”
They see opportunities. “Individuals who are concerned about their alcohol consumption could take OTC naltrexone, creating an opportunity for early intervention, even if they do not meet diagnostic criteria for AUD. While naltrexone has generally been recommended as a daily medication, studies support as-needed use of naltrexone (referred to as targeted use) prior to anticipated heavy drinking episodes to result in fewer drinks consumed. OTC naltrexone could become an adjunctive tool for those individuals attempting to cut back during Dry January or other temporary abstinence campaigns.”
They note four possible objections. Here, we focus on three:
Concerns for Liver Toxic Effects
“When naltrexone was initially approved for the treatment of AUD in 1984, a black box warning for hepatotoxic effects was required. However, the warning was removed in 2013 after data confirmed its safety. Evidence also supports naltrexone’s safety even when used by individuals with liver disease, including compensated cirrhosis. A widely used OTC medication, acetaminophen, is well known for its hepatotoxic properties yet is considered safe when used at recommended doses. In comparison, naltrexone has a relatively milder adverse effect profile and is well tolerated…”
Lack of Adjunctive Behavioural Treatment
“Given the overall underuse of MAUD, treatment for AUD is indeed centered around recommendations for psychosocial interventions, such as psychotherapy and peer support. While naltrexone is often used with adjunctive psychotherapy, its minimal use makes it an open empirical question as to whether OTC naltrexone alone can effectively support reduction in alcohol use. Similar concerns were raised with switching NRT from prescription to OTC. However, the effectiveness of NRTs in supporting smoking cessation is largely independent of the intensity of additional psychosocial support provided to the individual, leading a Cochrane review to conclude that ‘intense levels of support, although beneficial in facilitating the likelihood of quitting, is not essential to the success of NRT.’ Notably, it made it easier for physicians to recommend OTC NRT since patients can access it independently.”
Delay in Seeking Care
“Currently, only a small proportion of individuals with AUD seek care, estimated to be less than 10%. Moreover, individuals without AUD who want to moderate their drinking generally do not seek treatment. Nevertheless, to avoid potential delays in seeking care, OTC naltrexone could be paired with information about how and where to seek treatment resources, including self-guided programs.”
A few thoughts:
1. This is a thoughtful and creative paper on an important subject.
2. The comparison to smoking cessation (and OTC NRT) is particularly strong. If our tobacco strategy includes over the counter approaches, why would alcohol be so different?
3. Are the authors persuasive? Readers can draw their own conclusions.
4. Past Readings have included discussions of more access to medications. In a previous selection, Dr. Roy Perlis (of Harvard University) argued for over-the-counter antidepressants, noting that many people with depression are untreated. That Reading can be found here:
The full JAMA Psychiatry Viewpoint can be found here:
https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2840624
Selection 3: “Prevalence, magnitude and distribution of climate change anxiety in Canada: an interdisciplinary study”
S. L. Harper, A. Cunsolo, B. Aylward, et al.
Nature Mental Health, 21 October 2025

As climate change progressively and dramatically impacts livelihoods, culture, environments, infrastructure, economies and physical health around the world, people are increasingly experiencing a wide range of complex and nuanced emotions in response to the climate crisis. Climate change anxiety, in particular, has captured the attention of researchers and the media… Feeling anxious about climate change can be considered a rational, mature and healthy adaptive human response to the threats of climate change and can reflect a deep appreciation of a person’s interconnectedness with and reliance upon planetary health. Climate change anxiety can manifest in different ways, ranging from mild to severe cognitive and emotional impacts. Milder climate change anxiety includes occasional and less intense symptoms and has limited impacts on daily functioning… However, facing the complexity, uncertainty and vastness of the climate crisis can be unsettling. More extreme manifestations of climate change anxiety can reach clinical relevance and persist for longer periods of time. In these cases of severe climate change anxiety, daily functioning can be impacted, which can undermine well-being and agency, leading to hopelessness, burnout and apathy… This type of more severe climate change anxiety can be measured using Clayton and Karazsia’s Climate Change Anxiety Scale, which measures emotional elements, as well as rumination and functional impairment.
So begins a paper by Harper et al.
Here’s what they did:
- They conducted a national population-based cross-sectional survey – “using a multistage, multistratified random probability sampling method.”
- This included the Climate Change Anxiety Scale.
- They collected sociodemographic data.
- Statistical analyses were done.
Here’s what they found:
- A total of 2 476 individuals responded to the survey (response rate: 22.28%), conducted between 1 April 2022 and 31 March 2023.
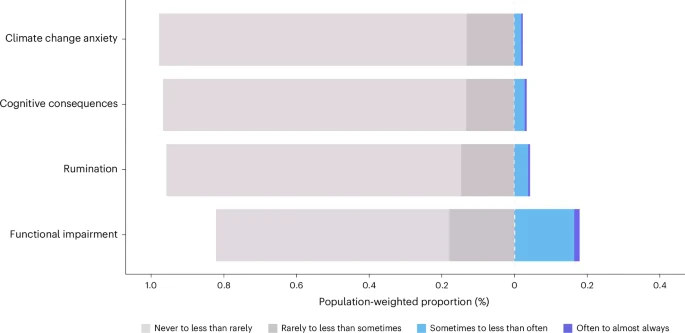
- Prevalence. “The population-weighted prevalence of experiencing symptoms of climate change anxiety that reach clinical relevance was 2.35%.”
- Gender. Women reported the highest prevalence of climate change anxiety (3.16%).
- Age. Climate change rumination was most pronounced among generations Y and Z (6.38%).
- Geography. People in the Northwest Territories had the highest prevalence of climate change anxiety, cognitive consequences, and rumination.
- Background. The prevalence of climate change anxiety for Indigenous Peoples (First Nations, Inuit, Métis and other Indigenous Peoples) was 9.63% – the highest prevalence of any demographic group in our survey.
A few thoughts:
1. This is an interesting paper on a timely topic.
2. The main finding: roughly 2.35% of people in Canada self-reported climate change anxiety.
3. Is this a disorder? A natural reaction to a global crisis? Or perhaps both? The authors offer perspective: “This is similar but slightly below the estimated annual prevalence of self-reported generalized anxiety disorder symptoms in Canada…”
4. Like all papers, there are limitations, including reliance on self-reported survey data.
The full Nature Mental Health paper can be found here:
https://www.nature.com/articles/s44220-025-00521-4
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments