From the Editor
“US Food and Drug Administration accepts only three outcome measures as primary endpoints in phase 3 studies to support an indication for major depressive disorder: the Hamilton Depression Rating Scale, the Montgomery-Åsberg Depression Rating Scale, or the Children’s Depression Rating Scale.”
The editors of The Lancet Psychiatry make this point in in the August issue of that journal. Their concern: the FDA view is very narrow and confined to these three scales.
In the first selection, we look at a new paper from The Lancet Psychiatry. Dr. Astrid Chevance (of the Center for Epidemiology and Statistics Paris Sorbonne) and her co-authors consider depression outcomes. To understand different perspectives, they draw on three groups: providers, patients, and caregivers. For the record, the resulting paper is fascinating and includes outcome measures that aren’t captured by these three scales. We consider the paper and the editorial that runs with it.

In the second selection – also on the topic of depression – Kashmir Hill and Aaron Krolik report for The New York Times on a popular therapy app. They note that Talkspace has good marketing and a growing client base. But should you recommend the app to your patients?
DG
“Identifying outcomes for depression that matter to patients, informal caregivers, and health-care professionals: qualitative content analysis of a large international online survey”
Astrid Chevance, Philippe Ravaud, Anneka Tomlinson, Catherine Le Berre, Birgit Teufer, Suzanne Touboul, Eiko I. Fried, Gerald Gartlehner, Andrea Cipriani, Viet Thi Tran
The Lancet Psychiatry, August 2020
Depression (depressive disorders and bipolar depression) is a frequent disorder, with a lifetime prevalence of about 15% – 18% and a mortality rate ratio of 2·07. This disorder is the fifth most common cause of years lived with disability worldwide. Despite thousands of trials of pharmacological and non-pharmacological interventions for depression, the clinical interpretation of results is still debated, because of two main reasons regarding the outcomes. First, the heterogeneity of outcomes, in terms of domains (what is measured) and measurement instrument (how the outcome is measured), limits the comparison and combination of results. For example, a meta-analysis comparing seven psychotherapeutic interventions for major depressive disorder across 198 studies identified 33 different outcome measurement instruments used in trials. Most of these instruments claimed to measure depression, but their content varied considerably. Second, we do not know whether the domains assessed in trials matter to people with a lived experience of depression (hereafter called patients, even though some might not have sought professional help), informal caregivers, and health-care professionals. Clinical trials of depression have been criticised for measuring domains that do not matter to patients…
 Astrid Chevance
Astrid Chevance
So begins a paper by Chevance et al.
Here’s what they did:
- The authors did an international online survey offered in three languages (French, German, and English).
- They surveyed adult patients with a history of depression, informal caregivers, and health-care professionals.
- “To capture the diversity of perspectives regarding what outcome domains are of value, we used purposeful sampling, targeting websites, and social media dedicated to depression.”
- People were asked four open-ended questions about their expectations for treatment.
- Four researchers independently then did qualitative content analyses.
Here’s what they found:
- The survey had 3 003 participants from 52 countries and five continents who completed the questionnaire: 1 912 (64%) patients, 464 (15%) informal caregivers, and 627 (21%) health-care professionals.
- Among 1 912 patients, 1 421 (75%) were women, with a mean age of 38.3 years, from 40 countries.
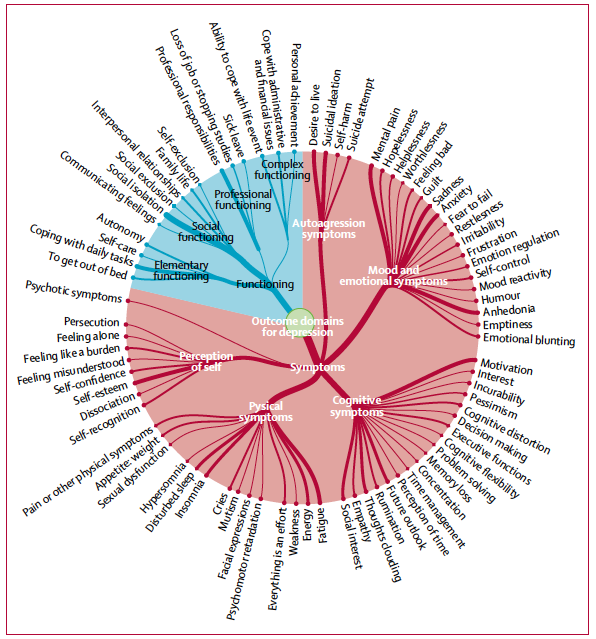
- They identified 80 outcome domains related to symptoms (64 domains), such as mental pain (or psychological or psychic pain, 17% of 3 003 participants) and motivation (13%), and functioning (16 domains), such as social isolation (18%). See below.
- They identified 57 other outcome domains regarding safety of treatment, health care organisation, and social representation, such as stigmatisation (14%).
A few thoughts:
- This is a good study.
- This is also an interesting study, in that it directly asked people (including patients) about outcomes.
- On this point, the authors write: “We identified functioning (e.g., capacity for patients to live a family life, get out of bed, be able to work) as a group of domains that matter to participants. However, functioning is not measured in six of the most used depression-rating scales… A cursory review of 90 meta-analysis of trials found that fewer than 5% of them reported functional outcomes…”
- And it wasn’t just functionality. The authors note: “Since domains were generated from the fine-grained descriptions of participants’ lived experience of depression, this study adds knowledge to their definition. Taking suicidal ideation as an example, participants considered several relevant dimensions, such as the intensity of suicidal ideation, the effort made to fight these ideas, and the emotional consequences (fear, guilt, shame, and psychological distress). These components do not align with how suicidal ideation is measured in common depression scales (or in the DSM-5 diagnosis of major depressive disorder), which highlights the importance of qualitative work involving stakeholders.”
- Like all studies, there are limitations. Among them: the self-reporting of depression.
- It’s also not clear how representative the sample is. Consider: 75% of patients came from one country (France). In terms of the severity of depression, most patients were more active in their symptom experience (66% were moderate or higher on the PHQ-9 scale).
- The paper runs with an editorial. The editors write:
“From 8 183 open-ended answers, Chevance and colleagues derived 137 domains of value to participants. The three most commonly mentioned domains were to raise awareness of society about depression, reduce the stigma of depression, and improve access to a psychiatrist. How often does one see these assessed even in socioeconomic studies, let alone clinical trials?”
The editorial concludes:
“Psychiatry has always faced difficulties in balancing the experiences of the individual against identifying common features that might guide research and treatment. The incorporation of lived experience into research projects should be standard practice: it is equally important to ask the right questions and to listen to the answers.”
That last comment is particularly thoughtful.
The editorial can be found here:
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(20)30302-3/fulltext
The paper can be found here:
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(20)30191-7/fulltext
“At Talkspace, Start-Up Culture Collides With Mental Health Concerns”
Kashmir Hill and Aaron Krolik
The New York Times, 7 August 2020
In 2016, Ricardo Lori was an avid user of Talkspace – an app that lets people text and chat with a licensed therapist throughout the day. A part-time actor in New York City, Mr. Lori struggled with depression and anxiety, and he credited the app with helping him get out of an abusive relationship. He was a believer in Talkspace’s stated mission to make ‘therapy available and affordable for all,’ and when the start-up offered him a job in its customer support department, Mr. Lori was ecstatic.
Talkspace, which has raised more than $100 million from investors, had an office in the old Studio 54 building in Midtown Manhattan, with all the usual perks – a Ping-Pong table in the conference room and beer and wine in the company fridge, plus all the therapy employees wanted. ‘I felt like I was at the best place in the world,’ Mr. Lori said.
After he wrote a general account of his therapy sessions on the company blog, an executive named Linda Sacco came to Mr. Lori with an intimate request. She wanted to give employees a sense of a typical user’s experience. Could she and one of the company’s co-founders, Roni Frank, read through two weeks of his therapy chat logs and then share excerpts with the staff?
 Kashmir Hill
Kashmir Hill
So begins an article by Hill and Krolik.
The article goes into detail on the success of Talkspace. According to The Washington Post, the number of clients has risen 65% since mid February.
It also details problems:
- “In 2015 and 2016, according to four former employees, the company sought to improve its ratings: It asked workers to write positive reviews. One employee said that Talkspace’s head of marketing at the time asked him to compile 100 fake reviews in a Google spreadsheet, so that employees could submit them to app stores.”
- “Karissa Brennan, a New York-based therapist, provided services via Talkspace from 2015 to 2017, including to Mr. Lori. She said that after she provided a client with links to therapy resources outside of Talkspace, a company representative contacted her, saying she should seek to keep her clients inside the app.”
- “The approximately 3,000 therapists who work on the platform are paid by ‘engagement,’ according to the company, based on the number of words they write to users or how often they talk by video or audio, with bonuses for client retention.”
- “According to multiple therapists, Talkspace paid special attention to their interactions with clients who worked at places like Google, Kroger and JetBlue — ‘enterprise partners’ that provide Talkspace to employees as a perk.”
- “Talkspace is advertised to users as unlimited, ‘24/7’ messaging therapy. ‘Your therapist will see your messages and respond to you throughout the day,’ the company says. Therapists get a different pitch: ‘Set your business hours, and check in on your clients daily, five days per week.’
The writers interview Hannah Zeavin, a lecturer in the English department at the University of California, Berkeley, who has written a book about teletherapy. “The app-ification of mental health care has real problems. These are corporate platforms first. And they offer therapy second.”
The article does include comments from people in the company. Neil Leibowitz, Talkspace’s chief medical officer, suggests that: “Talkspace has democratized access to therapy and psychiatry by meeting patients where they are in their lives and making treatment more affordable. The need is profound, especially now in this time of unease, and we are so proud of what our team of therapists is achieving.”
Returning to Lori, who watched Sacco and Frank read out a transcript of his therapy sessions:
“As Mr. Lori drank a tall glass of red wine and watched, he noticed that a few employees kept glancing his way. Afterward, a member of the marketing department approached and asked if he was OK. Later, Oren Frank, Ms. Frank’s husband and the chief executive, thanked him in the elevator. Somehow, word had gotten around that Mr. Lori was the client in the re-enactment.”
Lori – who was eventually terminated by the company and sued – notes that his privacy was breached.
A few thoughts:
- This is a good article.
- It should be noted that there is a total lack of data presented. That’s not a criticism of the NYT authors. The company didn’t provide the information. It’s difficult to judge an intervention with no data. The app seems to be commercially successful – but are people getting better?
- Zeavin makes a good point. The agenda of Wall Street (greater user engagement) is different than the agenda of clinicians (better outcomes).
- Patient privacy should include digital privacy – but doesn’t necessarily. Ouch.
The NYT article can be found here:
https://www.nytimes.com/2020/08/07/technology/talkspace.html
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments