From the Editor
Does investing in mental health make economic sense?
We often speak of mental health spending in terms of human terms – that people will have the opportunity to recover. But what about the economics of mental health?
 Economics & mental health: worth considering?
Economics & mental health: worth considering?
This week, we look at a new report from the Mental Health Commission of Canada. In it, the authors consider the impact of mental illness on our society, and then look at options for spending with an eye on economic returns.
In the other selection, we consider marijuana and public health with a blog by Dr. Gail Beck, a psychiatrist affiliated with The Royal. As Ottawa moves towards legalization, she offers a cautionary note: “Most physicians hope that the federal government will approach the legalization of marijuana emphasizing public health concerns as the most important consideration in the drafting of legislation.”
DG
Saving by Spending
“Strengthening the Case for Investing in Canada’s Mental Health System: Economic Considerations”
Mental Health Commission of Canada, March 2017

http://www.mentalhealthcommission.ca/sites/default/files/2017-03/case_for_investment_eng.pdf
In 2013, the Mental Health Commission of Canada released Making the Case for Investing in Mental Health in Canada, which set out a clear economic argument for investing in the mental health of people in Canada. With a cost to the Canadian economy of over $50 billion, 1.6 million Canadians reporting an unmet need for mental health care, and 7.5 million people in Canada living with a mental health problem or illness, the time for plans and strategies has long past. The time for action is now.
For the first time, the Government of Canada has made mental health a key priority in the new Health Accord. Momentum is growing to make wise investments in mental health.
Strengthening the Case is a crucial piece of the puzzle, clearly demonstrating how provinces and territories can bolster their bottom line while improving mental health outcomes. This win-win proposition makes the case that spending on mental health is an investment in our nation’s ‘mental wealth,’ rather than a drain on the public purse.
So begins a paper published by the Mental Health Commission of Canada.
The paper is really two papers: a consideration of the burden of mental illness on our society, and a paper reviewing the literature on ways of spending.
With regard to the burden, the paper makes several points:
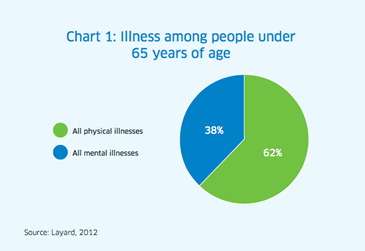
- “Mental health problems and illnesses are common. In 2016, more than 7.5 million people in Canada were likely facing one of the common mental illnesses — which is one in five Canadians, or more than the population of our 13 capital cities combined.” To emphasize the point, the authors draw from the work of British economist Richard Layard (see the graph below).
- “A person living with depression may experience at least 50% more disabling limitations in their life than someone with angina, arthritis, asthma, or diabetes.”
- “After unintentional injuries, suicide remains the second leading cause of death among young people ages 15-34.”
- “The MHCC estimates that the total cost to Canada’s economy incurred by mental health problems and illnesses is currently well over $50 billion annually, or nearly $1,400 for every person living in Canada in 2016.”
The authors then go on to highlight several studies showing the positive impact smart spending can have:
- “Community-based rapid-response teams, which can cut health care costs in half among young people experiencing suicidal thoughts.”
- “Improving access to psychotherapy, which creates improved quality of life and saves about two dollars for every dollar spent.”
- “Offering one session of counselling for high users of emergency rooms – the cost of which is offset from averted hospital visits and savings from earlier return to work – resulting in net savings of $21 per client in the first month.”
The authors conclude:
The Canadian studies and reports also illustrate and reinforce the spectrum of evidence-based interventions that align with priorities recommended in the 13 provincial/territorial mental health strategies, as well as in The Mental Health Strategy for Canada. They illustrate key priority areas that a majority of the strategies and plans share.
A few thoughts:
- This paper summarizes past work on the economic burden of mental illness, concisely and simply. Frankly, it makes for a powerful presentation.
- It’s great to see a consideration of the types of investments we could make in mental health services. For many years, the debate has been about whether to invest more in mental health (at present, Canada spends just 7 cents of every health dollars; the UK – to put that in perspective – spends 11 cents). But with federal-provincial deals ensuring an increase in spending, the debate has shifted, and this paper provides a nice context.
- The paper taps a rich literature. That said, the authors could have considered savings associated with better mental health services within hospitals. As hospital administrators focus more and more on metrics like length of stay, the burden of depression and delirium is better appreciated. Consider that the reason why the elderly man isn’t participating in his post-hip replacement physio may be because he is too depressed. The Birmingham RAPID study (UK), for example, found that psychiatric teams embedded within medical teams can shortened admissions and reduce readmissions.
Marijuana and Public Health
“How to Legalize Marijuana”
Gail Beck
drgailbeck.com, 9 April 2017
https://drgailbeck.com/category/my-blog/
My interview on CBC’s The House had such a positive reception that I wanted to follow up with a short essay summarizing most physicians’ recommendations for legalizing marijuana. My own perspective is that of a psychiatrist whose patients are all adolescents and young adults. This means I am concerned about the short-term impact of marijuana intoxication in the young people that I see, but I am even more worried about the long-term impact of cannabis on the developing brain as well as the links between cannabis use and psychotic illnesses.
Most physicians hope that the federal government will approach the legalization of marijuana emphasizing public health concerns as the most important consideration in the drafting of legislation. There are also law enforcement and government revenue aspects of the legislation but in jurisdictions where these considerations were emphasized, health outcomes were affected. Doctors in Canada – and Canadians in general – will find that negative health outcomes will eliminate any possible benefits to legalizing and regulating marijuana.
 Dr. Gail Beck
Dr. Gail Beck
So begins by a blog by Dr. Gail Beck, a psychiatrist affiliated with The Royal in Ottawa. Her writing is particularly timely given the federal government’s announcement that legalization will happen by 2018.
She makes several points about marijuana and legalization:
- “Some of the main health concerns with marijuana are related to its impact on the developing brain. The brain continues to develop until age 25 and there is significant evidence that cannabis use interferes with brain development. While it would be ideal if the minimum age to purchase marijuana could be 25…”
- “Child psychiatrists have also noticed increased prevalence of psychotic symptoms in young people using marijuana. We notice that psychotic symptoms emerge at a younger age for those with a predisposition for these conditions who use marijuana. We also notice that cannabis use is associated with the more serious chronic symptoms of schizophrenia.”
- “We notice that psychotic symptoms emerge at a younger age for those with a predisposition for these conditions who use marijuana. We also notice that cannabis use is associated with the more serious chronic symptoms of schizophrenia.”
- Beck also worries about intoxication while driving. “A method to evaluate intoxicationmust be developed before legalization. In this regard, the experience of Colorado should inform Canadian legislators. This excellent review outlines the increase in traffic accidents and Emergency Room visits since marijuana was legalized.”
She closes:
Benjamin Franklin made what must be one of the first public health statements in America. We can remember this as marijuana legislation moves forward, even if Colorado didn’t:
“An ounce of prevention is worth a pound of cure.”
 Ottawa and marijuana: considering the hazy future
Ottawa and marijuana: considering the hazy future
A few thoughts:
- Dr. Beck outlines reasonable public health concerns about marijuana legalization from the perspective of a practicing child psychiatrist. She offers thoughtful criticisms and suggestions, including comment on a “minimum age.”
- Of course, others have weighed in on this controversial issue. Ottawa’s recent announcement sparked much public debate.In terms of a well-researched and argued paper, CAMH published “Cannabis Policy Framework.” The authors do a nice job of noting the problems of cannabis use (which, they argue, “carries significant health risks”) with the problems of prohibition (which, they argue, confuses a public health issue with a legal one). You can find it here:
- Some will agree with these arguments, while others will disagree. I’ll remind you: Readings are about stoking debate.
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments