From the Editor
It’s a powerful tool that helps people with refractory depression and other illnesses.
It’s a treatment that carries a heavy stigma, and is used less today than even a decade ago.
Both statements describe electroconvulsive therapy (or ECT) – perhaps the most controversial intervention in psychiatry. And while it has been studied for decades, little work has been done considering the impact of ECT on inpatient readmissions. In this week’s Reading, we look at a new JAMA Psychiatry paper that studies ECT and readmissions.
Spoiler alert: the study authors found it decreased readmits.
 Electroconvulsive therapy at Winwick Hospital in 1957: relevant then as now?
Electroconvulsive therapy at Winwick Hospital in 1957: relevant then as now?
The paper begs a larger question: is an important tool in the treatment of those with mental illness being underutilized as newer (and less effective) treatments are chosen?
DG
ECT and Care
“Association of Electroconvulsive Therapy With Psychiatric Readmissions in US Hospitals”
Eric P. Slade, Danielle R. Jahn, William T. Regenold, Brady G. Case
JAMA Psychiatry, 28 June 2017
http://jamanetwork.com/journals/jama/article-abstract/2643308?resultClick=1
![]()
The limited and regionally variable availability of electroconvulsive therapy (ECT) in US hospitals is a curious phenomenon in view of ECT’s unique clinical benefits. Electroconvulsive therapy is considered the most efficacious treatment available for individuals with severe affective disorders, yet ECT is not used during inpatient care in nearly 9 of 10 US hospitals, and its use in these settings has declined over the past 2 decades. Factors speculated to impede ECT’s availability include stringent regulatory restrictions on its use, limited graduate medical training, persistent concerns among mental health consumers about ECT’s safety and adverse effects despite contemporary improvements in the procedure’s safety and adverse effect profile, stigma, reluctance among medical professionals to recommend ECT, and cost considerations. Electroconvulsive therapy also may be comparatively less accessible to individuals who live in rural and low-income urban areas, patients from minority racial/ethnic backgrounds, and those who have Medicaid insurance coverage or are uninsured. However, despite recent evidence that greater use of ECT may have important population health benefits, little research has examined whether the limited availability of ECT has any adverse effects on population health.
Research studies that demonstrate how the availability of ECT may affect health outcomes in a population are needed to help policymakers contextualize the need for ECT to be more accessible. Ahmadi and colleagues used a matched case-control study to compare outcomes for 92 patients with both major depressive disorder (MDD) and posttraumatic stress disorder from a large urban US Department of Veterans Affairs hospital who underwent ECT to the outcomes 3393 patients with MDD and posttraumatic stress disorder who did not receive ECT. During an 8-year follow-up period, ECT was associated with a lower risk of all-cause mortality and suicidality independent of antidepressant therapy utilization. To our knowledge, that study is the only such comparative effectiveness study in an entire patient population. However, as a consequence of its sample being drawn from a single Veterans Affairs hospital, its results have limited generalizability. Further research on ECT’s effects in broader population samples of hospital patients are needed to address this gap.
The present study used hospital inpatient census data from 9 states to examine whether greater ECT utilization results in fewer 30-day psychiatric inpatient readmissions among patients with severe affective disorders (ie, MDD, bipolar disorder, and schizoaffective disorder).
 Eric P. Slade
Eric P. Slade
So opens a new paper by Slade et al. considering ECT and inpatient admissions.
Here’s what they did:
- Drawing on data from the Health Care Utilization Project’s State Inpatient Database (SID) for 9 states, they looked at hospital stays, diagnoses, and demographics.
- Patients were 18 and over. They had to have a diagnosis of depression, bipolar or schizoaffective disorder.
- Readmission was defined as within 30 days of discharge.
- The authors looked at several co-variables, including demographics and hospital size.
- Statistical analyses were done. Given that patient’s getting ECT may be more ill, they did a “quasi-experimental model,” using an instrumental variables probit model to adjust. They also attempted to “weigh” length of stay between the ECT and non-ECT groups “to ensure valid mean comparisons of readmission risk because inpatient delivery of ECT is associated with longer-than-average stays, which in turn are associated with lower-than average readmission risk…”
Here’s what they found:
- Among the 162,691 inpatients, 2,486 (1.5%) underwent ECT during their index admission.
- Demographically: Those who received ECT were older (56.8 vs. 45.9), female (65.0% vs. 54.2%), and white (85.3% vs. 62.1%). Care tended to be in urban small hospitals (32.1% vs. 22.3%) and nonurban hospitals (9.0% vs. 7.6%).
- They tended to have to have MDD diagnoses (63.8 vs. 32.0%), not bipolar disorder or schizoaffective disorder.
- “Counterintuitively, ECT was administered more often to patients who had diagnoses indicating comorbid medical illnesses that may increase the relative health risks of ECT…”
- The mean length of stay in the ECT group was 20.7 days; for the no ECT group, it was 8.9 days before weighting and 20.6 days after weighting. !!
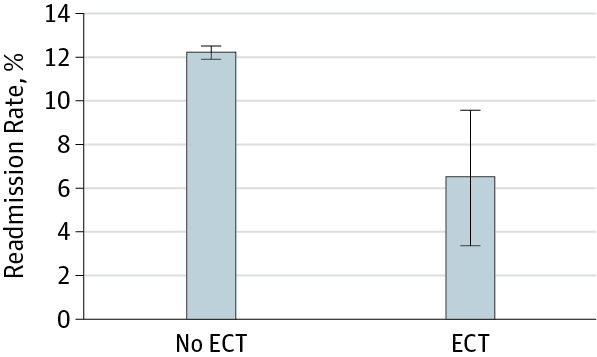
- A smaller proportion of the ECT group was readmitted within 30 days than in the non-ECT group – that is, 9.9% vs 12.2%. !! See figure below.
They note:
To our knowledge, this is the first study to examine how initiation of ECT during inpatient stays in US hospitals affects the likelihood of 30-day psychiatric inpatient readmission in a large, multisite sample of hospital inpatients diagnosed with severe affective disorders. Previous studies have found that treatment with ECT is associated with remission from depressive disorders and reductions in mortality in individuals with MDD and posttraumatic stress disorder. The results of the present study add evidence that wider availability of ECT may result in up to 46% fewer inpatient readmissions within 30 days of discharge among individuals with severe affective disorders. The effect of ECT on 30-day readmission risk did not differ significantly by age or race/ethnicity but was relatively larger among men than women and among individuals with bipolar disorder and schizoaffective disorder than among those with MDD.
The paper runs with an editorial, “Modern Electroconvulsive Therapy: Vastly Improved Yet Greatly Underused.” (What a great title, by the way.) You can find the paper here: http://jamanetwork.com/journals/jamapsychiatry/fullarticle/2633172
 Harold A. Sackeim
Harold A. Sackeim
Columbia University’s Harold A. Sackeim reviews the history of ECT, and the strong clinical evidence for this intervention.
To my knowledge, no treatment, pharmacological or otherwise, has matched ECT in speed or likelihood of remission of major depressive episodes. Electroconvulsive therapy is equally effective in unipolar and bipolar depression and has profound antimanic properties.
He then focuses on the Slade et al. paper.
Perhaps the most important contribution of this study is documentation of the extraordinarily low rate of ECT use and the demographic characteristics of those who receive it. Previous research demonstrated marked geographic variability in ECT availability, and nearly 9 of 10 US hospitals do not offer this treatment. Slade et al found that while the percentage of inpatients receiving ECT was small (1.5%)…
A few thoughts:
- This is a good study.
- This paper has implications on care and the way we organize care. ECT has fallen out of fashion – but is that consistent with the best evidence? Slade et al. looked at rehospitalizations, an important metric; there are many reasons why we would want to avoid rehospitalizations, including the stress on patients themselves. Consider this, though, from an economic perspective: inpatient hospitalizations are very expensive. Going back to the major finding of the paper: “up to 46% fewer inpatient readmissions within 30 days of discharge among individuals with severe affective disorders.” Wow. The authors didn’t do an economic analysis, but it would seem that the longer length of stay for the ECT group is well compensated for by the drop in readmissions (especially in light of the “weighing” calculations done by the authors).
- Building on that last point: Many hospitals don’t even offer ECT, according to this study; how many seek to inform and educate patients on this option? One would suspect few.
- There are obvious limitations to this study. The authors did a “quasi-experimental model;” the intervention (ECT vs. no ECT) wasn’t randomized – as Sackeim points out eloquently in his editorial. And we don’t know much about the patients themselves beyond demographics. What is their pre-admission functionality like? How many of them have psychotic illness? Etc. Still, the paper nicely points out that there is a trend in practice – few (and declining) ECT treatments among inpatients – and a problem with it – that is, ECT reduced readmissions.
- But does the evidence mater? In the age of YouTube and Twitter, when the brutal portrayal of ECT in One Flew Over The Cuckoo’s Nest is a click away, is electroconvulsive therapy doomed to the ash heap of history?
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments