From the Editor
Is new better?
You may be reading this on an iPhone 7, having driven to work this morning in a 2017 Hybrid Prius. So should your patients be taking a medication that became available four-and-a-half decades ago – when people drove gus-gusling eight-cylinder Oldsmobiles and smartphones didn’t even exist in science fiction novels.
This week, we look at a just-published JAMA Psychiatry paper which promises to look at the “real-world” effectiveness of antipsychotics. The authors tapped Swedish databases to consider outcomes for nearly thirty thousand people with schizophrenia.
 Sweden: elaborate welfare state, beautiful historic buildings, and – yes – rich databases
Sweden: elaborate welfare state, beautiful historic buildings, and – yes – rich databases
Spoiler alert: new wasn’t better. That is, newer antipsychotics tended to underperform clozapine and depot medications.
We also look at similar “real-world” work drawing from a Finnish database considering treatment of depression.
DG
Antipsychotics and Outcomes
“Real-World Effectiveness of Antipsychotic Treatments in a Nationwide Cohort of 29 823 Patients With Schizophrenia”
Jari Tiihonen, Ellenor Mittendorfer-Rutz, Maila Majak, Juha Mehtälä, Fabian Hoti, Erik Jedenius, Dana Enkusson, Amy Leval, Jan Sermon, Antti Tanskanen, Heidi Taipale
JAMA Psychiatry, 7 June 2017 Online First
http://jamanetwork.com/journals/jamapsychiatry/article-abstract/2629295
![]()
The comparative effectiveness of antipsychotic treatments for patients with schizophrenia has remained controversial despite extensive research. Results from randomized clinical trials (RCTs) suggest that clozapine, olanzapine, and amisulpiride are superior to other antipsychotic medications in terms of efficacy. However, the most efficacious drugs such as clozapine and olanzapine frequently induce adverse effects, such as weight gain and dyslipidemia, which may result in severe deterioration of health after long-term treatment. Investigation of these adverse effects or associated outcomes such as hospitalization and death requires thousands of patients and several years of follow-up to achieve enough statistical power, which is not possible for RCTs.
Another major issue in RCTs is the selection of patients. Those included in RCTs represent an atypical minority of the patient population because up to 80% to 90% of patients are excluded because of refusal, substance abuse, suicidal or antisocial behavior, or mental or physical comorbidity. Especially problematic is the comparison of oral antipsychotic medications vs long-acting injections of antipsychotic medications because patients with the poorest adherence (ie, those who would receive the greatest benefit from long-acting injectable antipsychotic medications) are excluded from RCTs because participation is fully voluntary. Because RCTs include only an atypical fraction of the most adherent patients, they do not provide information on the real-world effectiveness of the antipsychotic treatments.
 Jari Tiihonen
Jari Tiihonen
So opens a new paper by Tiihonen et al. In this paper, the authors make an observational study, drawing on national databases. This approach isn’t unique – the authors acknowledge past work shows better outcomes for clozapine, olanzapine and long-acting depot medications – but such work has had the problem of selection bias.
They attempt to address this:
We aimed to overcome this problem by using within-individual analysis, in which each person is his or her own control. In this approach, the exposure periods of each individual are compared with the nonexposure periods of the same individual. Therefore, the only factors that need to be adjusted are those that change as a function of time, such as time since cohort entry, temporal order of exposure periods, and concomitant medications.
Here’s what they did:
- “We used nationwide register-based data to conduct a prospective population-based cohort study of patients with schizophrenia…”
- Drawing on Swedish databases, they looked at people with a diagnosis of schizophrenia between July 1, 2006, to December 31, 2013. Inclusion criteria included “all individuals residing in Sweden who were 16 to 64 years of age in 2006.”
- Data on medication use was drawn from the Prescribed Drug Register – which includes outpatient medication, though no inpatient prescriptions. (!)
- They considered outcomes as follows: “psychiatric rehospitalization” and “treatment failure” (defined as rehospitalization, discontinuation or switch to other antipsychotic medication, or death).
- They did a more complicated statistical analysis – that is, they used within-individual Cox proportional hazards regression model. “The within-individual model is a stratified Cox proportional hazards regression model in which each individual forms his or her own stratum.” They also looked at covariables.
Here’s what they found:
- There were 29,823 patients.
- Demographically: more men than women (12,822 women and 17,001 men). The mean age was 44.9.
- “13,042 of 29,823 patients (43.7%) experienced psychiatric rehospitalization and 20,225 of 28,189 patients (71.7%) had treatment failure.”
- In terms of drugs used: Oral olanzapine was the most frequently used drug, and zuclopenthixol the most frequently used as a long-acting injectable antipsychotic medication.”
- In terms of rehospitalization: “The lowest risk of rehospitalization was observed for once-monthly long-acting injectable paliperidone (HR, 0.51), long-acting injectable zuclopenthixol (HR, 0.53), clozapine (HR, 0.53), long-acting injectable perphenazine (HR, 0.58), and long-acting injectable olanzapine (HR, 0.58).” See figure below.
- In terms of treatment failure: “The lowest risk of treatment failure was observed for clozapine (HR, 0.58), and the second lowest was seen for all long-acting injectable antipsychotic medications (HRs, 0.65-0.80), whereas the highest risk was seen for levomepromazine (HR, 1.15).” See figure below.

Adjusted Hazard Ratios (HRs) and 95% CIs for Psychiatric Rehospitalization During Monotherapy Compared With No Use of Antipsychotic in Within-Individual Analyses in the Prevalent Population
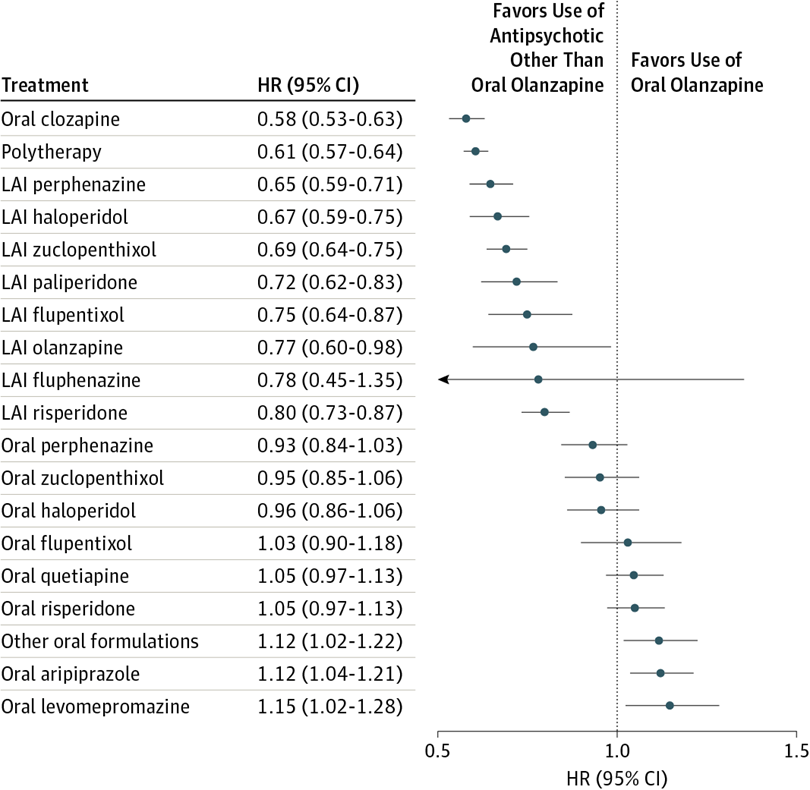
Adjusted Hazard Ratios (HRs) and 95% CIs for Treatment Failure During Each Monotherapy Compared With Oral Olanzapine Use
Our results from a large nationwide cohort show that clozapine and long-acting injectable antipsychotic medications are substantially more effective than other antipsychotics in reducing the risk of rehospitalization or any treatment failure. The most consistent findings were observed for clozapine, being the first in rank order in most of the analyses. These results are in line with those of previous cohort studies using traditional between-individual analyses, although the effect sizes differed to some extent, especially for comparisons between long-acting injectable antipsychotic medications and corresponding oral formulations. Our results showed that the risk of rehospitalization was 22% lower during treatment with long-acting injectable antipsychotic medications compared with treatment with equivalent oral formulations in the total cohort and 32% lower in the incident cohort of newly diagnosed patients.
A few thoughts:
- This is a good study, drawing on a huge dataset – not dozens of people with schizophrenia, or even hundreds, but tens of thousands.
- The findings are strong. Let’s not mince our words: new isn’t necessarily better. Of the five best performing medications for treatment failure that were studied, four were old. And, yes, clozapine topped that list. Depot medications were very strong in terms of rehospitalizations, with robust results for drugs that pre-date Atari’s Pong (the first and only video game in 1972), like perphenazine; though it should be added that paliperidone (new) did the best.
- There are implications here for practice – how many newly diagnosed patients are on depot medications? There are also implications in terms of health systems – does funding and billing schedules reward depot choices over non-depot choices? Dare I ask about clozapine?!?
- Has similar work been done for depression? Actually, Lancet Psychiatry has a solid paper with a very similar analysis. That’s not exactly surprising since Tiihonen is the first author. (Wow, he’s having a good month, at least compared to Theresa May.) In this study, he and his co-authors tap Finnish databases. I will quickly summarize “Pharmacological treatments and risk of readmission to hospital for unipolar depression in Finland: a nationwide cohort study”: they looked at the risk of readmission for all patients who had at least one hospitalization for depression, with data from almost 125,000; exclusion criteria included schizophrenia and bipolar. They found: “Lithium use was associated with a lower risk of re-admission to hospital for mental illness than was no lithium use.” Yes, lithium – speaking of older medications, this one is as old as the earth.

- In the accompanying editorial, Allan H. Young of King’s College is enthusiastic about the findings, but calls for more investigation into lithium:
Replication of these findings is needed, and should be possible given that similar databases exist in other countries (e.g., Denmark and Taiwan). These data could be easily assessed to establish whether they replicate the Finnish findings or not. The findings of Tiihonen and colleagues are particularly noteworthy because of recent disquiet about the use of antidepressants in unipolar mood disorders, and they suggest that lithium monotherapy might be the best long-term prophylactic drug.
- Big data is changing psychiatry.
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments