From the Editor
Substance work can be lifesaving. But it’s also challenging, as many patients continue to misuse illicit drugs or drop out of care or both. Evidence supports using incentives, including financial ones, to nudge patients toward sobriety. This approach, known as contingency management, includes tools such as vouchers and prizes.
But what forms of nudging work best? And how much of a financial incentive is needed? In a new JAMA Psychiatry paper, Carla J. Rash (of the University of Connecticut) and her co-authors attempt to answer these questions by looking at contingency management. In a systematic review, they drew on 112 protocols from 77 studies, analyzing types of nudges like vouchers (which may be exchangeable for, say, retails items) and prizes (a chance to win things like gift cards) and the amounts of money involved. The authors walk on a familiar path – the literature goes back four decades – but provide a meaningful update. “Based on these findings, weekly incentive magnitude estimates are $128/week for voucher protocols and $55/week for prize-based protocols.” We consider the paper and its implications.

ChatGPT is the most downloaded app in history with people using it for everything from finding recipes to writing emails. How could generative AI be used for mental health? In a perspectives paper for The Lancet, Drs. John Torous (of Harvard University) and Eric J. Topol (of the Scripps Research Translational Institute) discuss this important and timely topic. “Despite considerable promise, research is still required to establish AI’s benefit and safety for promoting mental health.”
And in the third selection from Academic Psychiatry, Dr. Ariel E. Wilson, a resident of psychiatry at Kaiser Permanente Oakland, writes about patient rights, certifiability, and the weight of making good decisions. The author asks if psychiatrists need to have thick skin. “The challenge in psychiatry lies in finding a balance – creating our own semi-permeable membrane that allows us to protect ourselves from feeling the sting of every emotion we encounter, while also maintaining empathetic and trusting relationships with our patients.”
DG
Selection 1: “Data-Driven Contingency Management Incentive Magnitudes: A Review”
Carla J. Rash, Sonata I. Black, Sara C. Parent, et al.
JAMA Psychiatry, 2 July 2025 Online First

Contingency management (CM) interventions have more than 40 years of research support as a treatment for stimulant and other substance use disorders, patient population characteristics, and clinical settings. Despite robust research evidence, clinical implementation of CM for stimulant use disorders has been limited in the United States. The Department of Veterans Affairs (VA) initiated the first large-scale clinical rollout of CM in the US in 2011. This effort was successful in reaching patients with stimulant use disorders and continues today. More recent efforts involve the California Recovery Incentives Program, which in just under 2 years has trained 100 sites in 19 counties and has reached more than 5000 patients, as well as other statewide pilots and regional efforts.
CM magnitude is directly related to its efficacy, but little guidance on CM magnitudes is available. As CM continues to expand, it is important that stakeholders support CM programs of sufficient magnitude to reduce substance use. Many of the seminal studies of CM were conducted decades ago… CM research protocols vary in duration, magnitude, behavioral targets, models, and settings; thus, no single recommended magnitude exists.
So begins a paper by Rash et al.
Here’s what they did:
- They conducted a review to “provide data-driven inflation-adjusted incentive estimates for modern CM protocols.”
- They reviewed published meta-analyses and review articles focused on CM that included randomized clinical trial with a non-CM comparator condition and CM protocol involved reinforcement of negative stimulant and/or opioid.
- They “excluded studies focused on tobacco, alcohol, or cannabis because their CM protocols are often structured differently.”
- They extracted effect sizes and analyzed them.
Here’s what they found:
- There were 112 protocols.
- Reinforcement. 44% reinforced stimulant-negative urine drug tests (UDTs) only, 6% reinforced opioid-negative UDTs only, 21% reinforced both stimulant- and opioid-negative UDTs, and 29% reinforced additional drugs beyond stimulants and/or opioids (like alcohol).
- Behaviours. Most (81%) reinforced only negative UDTs. 5% reinforced both negative UDTs and treatment attendance, 5% reinforced both negative UDTs and treatment goal–related activities, 5% targeted both negative UDTs and medication adherence.
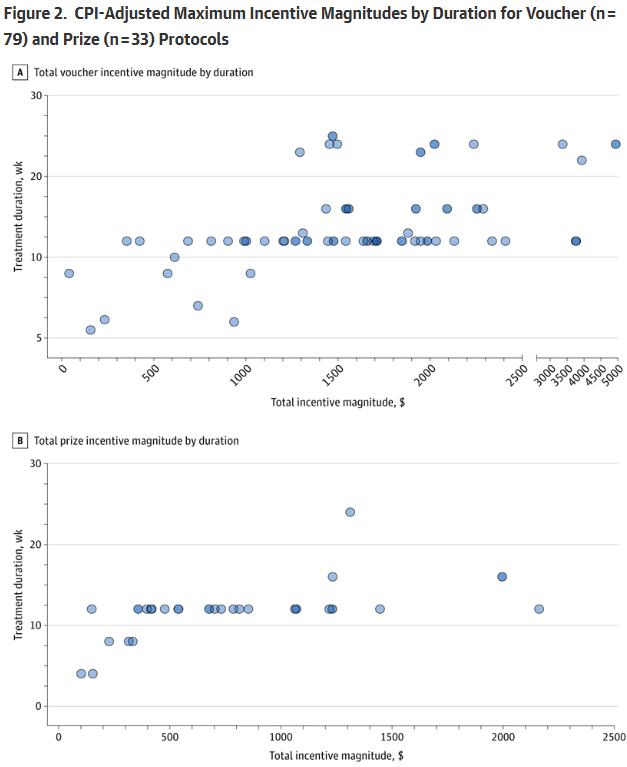
- Vouchers and prizes. Voucher protocols ranged from $25 to $5800 with a median value of $1034 and modal value of $1155. Prize protocols ranged from ranged $65 to $1460 with a median and modal value of $420. See figures below.
- Amount. “Data-driven weekly estimates are $128 for voucher protocols and $55 for prize protocols”
A few thoughts:
1. This is a good paper on a relevant problem, and published in a major journal.
2. The main finding in a sentence: “In this systematic review, data produced inflation-adjusted weekly median magnitude estimates of $128/week for voucher protocols and $55/week for prize protocols. For the most common duration of 12 weeks of incentive delivery, these estimates translate to $1536 for voucher and $660 for prize protocols.”
3. The authors put these amounts into perspective: “weekly estimates for first-line treatments approved by the US Food and Drug Administration for opioid use disorder delivered in opioid treatment programs are $126/week for methadone treatment, $115/week for buprenorphine, and $271 for injectable naltrexone.” They also do comparisons with other types of treatment: “costs attributable to diabetes are about $231/week and for chronic kidney disease, about $261/week.” They add: “The costs of CM incentives are comparable or less than these treatments, and in contrast to these treatments, CM is typically time-limited as currently delivered, and costs are not perpetual.” (!!)
4. To state the obvious: the amount of money isn’t great. (And there is more to life than the cost-benefit analysis. Successful substance treatment, after all, may immeasurably improve the quality of a person’s life.) The idea of nudging has gained popularity since publication of Richard H. Thaler and Cass R. Sunstein’s bestselling book. Is it time for contingency management to enjoy a moment?
5. Like all studies, there are limitations. The authors note several, including that they “relied on author-reported protocol details, including magnitude, which may be subject to error.”
6. There is something very reassuring about this study, suggesting that an evidence-based intervention isn’t heavy financially in the overall scheme of things. This study, though, is a bit simplistic. After all, evidence suggests that incentives should increase over the course of a patient’s treatment and be part of a larger care package; the figures are, thus, crude.
The full JAMA Psychiatry paper can be found here:
https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2836114
Selection 2: “Assessing generative artificial intelligence for mental health”
John Torous and Eric J. Topol
The Lancet, 11 June 2025 Online First

As more studies emerge exploring the potential of artificial intelligence (AI) conversational chatbots in health, it is clear these tools offer benefits that were absent in earlier digital health approaches. The generative abilities of newer chatbots have surpassed the previous generation of rule-based chatbots and mental health apps in their ability to gain medical knowledge, synthesise information, customise care plans, and potentially be scaled up for use in mental health services. Earlier this year the first randomised trial of a generative AI chatbot (Therabot) for mental health treatment was reported. The Therabot intervention was compared with a waiting-list control in adults with major depressive disorder, generalised anxiety disorder, or at risk of feeding and eating disorders and showed symptom improvement at 4 and 8 weeks. Yet larger trials and more research are warranted to confirm the effectiveness and generalisability of this and related chatbots interventions.
In the face of such transformative potential, it is useful to identify and support the most promising uses of AI chatbots while remaining vigilant about AI hype. Even health regulators, such as the US Food and Drug Administration, struggle to navigate this space because of its rapid changes.
So begins a paper by Drs. Torous and Topol.
They propose three considerations that can “help guide informed decision making on the potential of any AI chatbot.”
Any claims should be considered in the context of the quality of the supporting evidence. A decade of digital health work in smartphone apps has shown the risk of comparing apps to waiting-list controls (an untreated comparison group)
“Intervention research done without a placebo or active control group is still important but should be considered more preliminary in the same way that early-phase drug studies explore feasibility and safety rather than efficacy. Comparing an AI chatbot to nothing, or a waiting-list control, can be questioned given the range of online, app, augmented reality, virtual reality, and even other AI interventions that can serve as active digital control.”
Another area for caution concerns the longitudinal impact of AI tools
“While achieving immediate and short-term symptom reduction is important, most health-care needs require longitudinal benefits. Similarly, economic analyses of the cost savings of AI tools are typically forecasted around their potential to deliver long-term outcomes. Today’s digital therapeutics and health apps have struggled with long-term outcomes as well as sustained engagement among people who use health-care services. It might be possible that AI tools can deliver such effective interventions that sustained engagement is not necessary or the intervention might be able to drive ongoing engagement such that the user receives ongoing longer-term support. These areas need further research.”
Any claims that generative AI is therapeutic need to be placed in the broader context of treatments, including medical liability
“If an AI intervention is unable to assume the legal responsibility and risk associated with clinical care, then it cannot deliver care. At the present time, for generative AI to support mental health, there still needs to be a role for health professionals to monitor patient safety. Indeed, leaving the responsibility and risk on humans suggests AI alone cannot deliver care. Thus, developments in the legal and regulation space will prove crucial for ensuring AI tools have a genuine role in health care.”
A few thoughts:
1. This is an interesting and important commentary.
2. The comment about wait-list controls is particularly important. As has been noted in a past Reading (quoting Dr. Torous), Tetris can beat wait-list controls.
3. Is today’s enthusiasm greater than our current reality? Drs. Torous and Topol argue yes, a reasonable conclusion, especially in a week with news reports that Grok, a popular AI chatbot, wrote fondly about Hitler.
4. Interested in voicing your opinion on AI and medicine? Dr. Torous and Dr. Eric Achtyes (of Western Michigan University) are studying physician attitudes to AI. They ask physicians to complete a confidential survey. Time ask: about ten minutes. See:
The full Lancet perspectives paper can be found here:
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(25)01237-1/fulltext
Selection 3: “Thick Skin”
Ariel E. Wilson
Academic Psychiatry, June 2025

‘Being a psychiatrist requires a thick skin,’ my attending told me. It was my first rotation as a psychiatry resident at an inpatient psychiatric hospital, and a patient had just yelled profanities at me after I told them that I did not feel they were ready to be discharged from the hospital. I felt a stab of fear in my stomach at my attending’s words. I had never thought of myself as having thick skin, in fact quite the opposite. I was sensitive to how others perceived me, wanted to please others, and always felt obligated to help balance others’ emotional states. Did this mean I was not cut out to be a psychiatrist?
My doubts continued as I was struck by the full force of the responsibility to place patients on psychiatric holds. Could he care for himself on his own, or would he end up on the street again with no belongings because the voices in his head told him to give everything away? If she left the hospital, would she hurt herself, or was she no longer suicidal?
So begins a paper by Dr. Wilson.
She notes the complexity of such decisions around patient rights. “I was only seeing a snapshot of their lives but needed to make a monumental decision. It seemed clear that I was doing the right thing when patients were severely impaired, such as a patient with psychosis who would not eat because he believed his food was poisoned. But what about the mother with mania who had children that she desperately wanted to get home to – was she too disorganized to care for her children? At what point was I helping her versus hurting her or her children? The gray areas were the hardest to cope with.”
She takes some comfort in the failure of patients to win appeals: “Patients rarely won.” She notes: “Perhaps that provided some validation. After all, an objective third party agreed with my decision. But the imbalance of power was not lost on me…” That said, she adds: “I had envisioned entering psychiatry to help those who were seeking help but had thought less about encountering situations where my help was not wanted. The therapeutic alliance that I tried so hard to maintain often became shattered and irreparable.”
Further along in training, she now feels more settled in these decisions. “I still feel the weight of these decisions, although it feels less heavy the longer I have carried it. I have seen plenty of good outcomes to recognize that the system can work, but it does not work for everyone.”
Is thick skin the solution? “I do not think that the solution is to grow a ‘thick skin’ so that patients’ words bounce off us into the ether as though they bear no further reflection. It may feel tempting as a short-term solution, a way to maintain the strength to carry on our appreciably difficult duties as psychiatrists. However, I fear that growing a thick skin will only create more walls between us and our patients, amplifying the distance and reinforcing the barrier between ‘us’ and ‘them.’ This sort of detachment jeopardizes the patient-psychiatrist relationship by minimizing the weight of our decisions and diminishing the empathy we have for our patients.”
A few thoughts:
1. This is a well-written essay that raises good points.
2. Dr. Wilson wrestles with the implications of certifiability – and we all should.
3. This comment is thoughtful and worth repeating: “I fear that growing a thick skin will only create more walls between us and our patients…”
The full Academic Psychiatry paper can be found here:
https://link.springer.com/article/10.1007/s40596-024-02077-4
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments