From the Editor
At times, it seems that we understand little about suicide.
That statement is vast, sweeping – and painfully true for us clinicians who aspire to do better with very blunt instruments. This week, we have three selections; the first is a systematic review and meta-analysis focused on suicide. In a new Canadian Journal of Psychiatry paper, Rebecca Barry (of the University of Toronto) and her co-authors consider the potential link between suicide and rurality. Spoiler alert: they find a connection, at least for men. What are the implications for practice and policy?

In the second selection, we consider a new podcast discussing our digital future. I talk with Dr. Jay Shore (of the University of Colorado), who chairs the APA’s Telepsychiatry Committee. We discuss the virtualization of mental health services, and contemplate a future of hybrid care. And, yes, he has tips on how to avoid “Zoom fatigue.”
In the third selection, activists Asante Haughton and Rachel Bromberg discuss alternatives to police responding to mental health crises, seeing a dedicated team tasked with “on-the-spot risk assessments, de-escalation, and safety planning for clients in crisis” and more. “By taking on these important tasks, this team will enable Toronto policing resources to be more effectively directed toward solving crimes, rather than providing social services.”
DG
Selection 1: “Rurality and Risk of Suicide Attempts and Death by Suicide among People Living in Four English-speaking High-income Countries: A Systematic Review and Meta-analysis”
Rebecca Barry, Jürgen Rehm, Claire de Oliveira, Peter Gozdyra, and Paul Kurdyak
The Canadian Journal of Psychiatry, July 2020
![]()
Over 800,000 people die from suicide worldwide each year. For every completed suicide, there are many more suicide attempts. Differences in suicide rates across the rural–urban continuum have been observed in studies across many countries including Canada, the United States, Australia, and the United Kingdom (UK). The reason for this rural–urban disparity is unknown, but several theories have been proposed such as physical and social isolation, access to firearms, decreased access to mental health and other health services, attitudes or stigma toward mental illness and help-seeking behaviors, and misclassification of cause of death. The association between rurality and suicide has not been systematically reviewed to date.
The primary objectives of this review are to determine (1) whether those living in rural areas are more likely to complete suicide than those living in more urban areas and (2) whether those living in rural areas are more likely to attempt suicide than those living in more urban areas.
So opens a paper by Barry et al.
Here’s what they did:
- They conducted a systematic review and meta-analysis of observational studies.
- They included studies from four countries: Canada, the United States, the United Kingdom, and Australia.
- Data sources included various databases including PubMed. Both published and unpublished literature was included in the search.
- Publications were included that were published between January 1, 2006 and December 31, 2017.
Here’s what they found:
- With the initial search terms, there were 6 259 citations. 53 studies were ultimately found to be consistent with the aims of the systematic review.
- 9 were from Canada.
- Outcome: completed suicide. “Of these, 30 studies suggest that those living in rural areas have a higher risk of completed suicide, with 12 of these indicating that only rural males have an increased risk of suicide.”
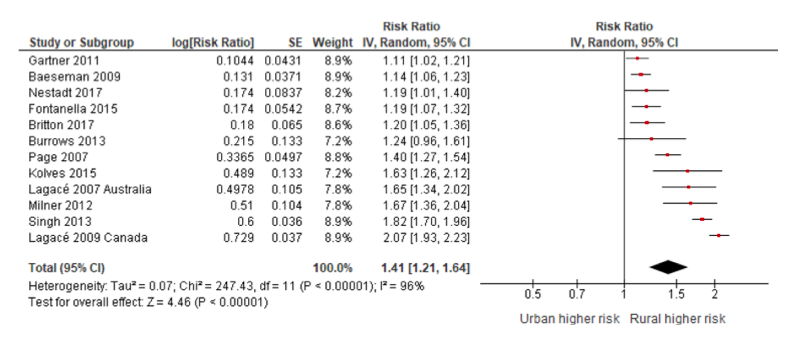
- “The meta-analysis indicates that among those studies which report suicide for the entire population (male and female combined), suicide is higher among rural populations (RR = 1.22…). Among those that report estimates for males, rural males are more likely to complete suicide than urban males (RR = 1.41…).” See figure below. Rural females, however, weren’t at higher risk than their urban counterparts.
- Outcome: attempted suicide. “Of the studies included in this review, 11 studies examine suicide attempts by rural–urban status… Of these, 3 suggest that rural areas have higher rates of suicide attempts, and 1 suggests that only rural females have higher rates.”
- “The meta-analysis indicates that there are no differences between rural and urban areas in terms of suicide attempts (RR = 0.93…).”
 “Overall, the results suggest that rurality is associated with increased risk of completed suicide. Furthermore, the results suggest that sex may be an effect modifier of this association, with rural males being at greater risk of suicide than urban males, while females may be at a similar risk, regardless of residence.”
“Overall, the results suggest that rurality is associated with increased risk of completed suicide. Furthermore, the results suggest that sex may be an effect modifier of this association, with rural males being at greater risk of suicide than urban males, while females may be at a similar risk, regardless of residence.”
This is a good study, and there is much to like here, including that it covered studies in four countries.
Why the difference in rural vs. urban suicides for men? The authors comment: “One possible reason for the sex effect modification is less access to formal mental health care in rural areas. This lack of access may be more detrimental to males in rural areas because emotionally supportive relationships are substantially more protective against major depression for women than for men. Another potential explanation is that males in rural areas are likely to be employed in occupations such as farming or forestry, which are associated with higher risk of suicide.”
The authors see implications for practice and public policy:
“Our systematic review shows that those living in rural areas are at increased risk of suicide in comparison to their urban counterparts and that this association is particularly strong among males. Family physicians and psychiatrists practicing in rural areas or in urban areas with rural catchment areas should be aware of this important risk factor when assessing their patients’ overall risk of suicide. Medical professionals involved in education should be aware of this risk factor when educating family physicians in rural communities as well as gatekeepers in rural communities (e.g., teachers, police officers, spiritual leaders). Public health campaigns focused on suicide prevention that currently only target urban areas should consider how they can reach rural populations as well.”
A couple of thoughts:
- These are practical suggestions, and actionable.
- We can wonder if the virtualization of mental health services has improved the access to care for those in rural areas (providers can be seen with less travel) or worsened it (some 30 million North Americans lack access to broadband with disproportionately many in rural areas).
This CJP paper can be found here:
https://journals.sagepub.com/doi/10.1177/0706743720902655
Selection 2: “What all physicians need to know about the rapid virtualization of mental health care – and the post-pandemic future”
Jay Shore and David Gratzer
Quick Takes Podcast, 8 July 2020

COVID-19 has brought a rapid virtualization of mental health care. What to make of it all? And what will our post-pandemic future be like? I sat down with Dr. Jay Shore to discuss.
On the changes to mental health care during COVID-19:
“We’re having a digital moment probably in medicine and behavioural health like one we have we have never seen…
“In February 2020, telepsychiatry was widespread in its use, but diffuse and sporadic. Some systems were doing a fair amount, and some systems weren’t really using it. And, of course, in March, that radically changed. And it’s difficult to think of a provider or an organization that I know or work with that isn’t using some form of telepsychiatry.”
On the post-COVID world:
“We are beginning to try and understand this concept of hybrid care, which is the concept that we hold as providers, but even as human beings in our individual lives. You know, we manage relationships through multiple different mediums and technology. So I have relationships with people in person, over video, over telephone, texting, patient portals, social networking.
“And so you have to understand how to use the technologies to form good, strong relationships for clinical care, trying to understand which technology they use with which patient and when.”
On (three) tips for avoiding “Zoom fatigue:”
“Create space in your day to go for a 30 minute jog or a walk. Build in those little breaks…
“When you’re working at home alone, you rely a little more heavily on email and texting and not casual conversations. So pick up the phone and talk to two to three minutes with a colleague… Shoot them a message and then get on the phone…
“Make sure that you do get some training on the technology you’re using.”
 Interviewing Dr. Shore (virtually, of course)
Interviewing Dr. Shore (virtually, of course)
The podcast can be found here, and runs just under 20 minutes:
https://www.porticonetwork.ca/web/podcasts/quick-takes/virtualization#QT
Selection 3: “The alternative to calling the police during a mental health crisis”
Asante Haughton and Rachel Bromberg
The Toronto Star, 2 July 2020
![]()
Someone you care about is struggling and you don’t know what to do. Perhaps they’ve been hearing distressing voices, or thinking about suicide and they need help. You’ve tried talking to them, offered suggestions, listened. But nothing has worked. It’s getting worse. Your loved one needs more than you can offer.
So you call 911.
Within minutes, police are at your door. They knock in the loud way only police officers knock. Your adrenalin rushes, a response usually reserved for encounters with danger. You open the door to find two officers. You notice their Kevlar vests, their hands by their belts, unnervingly close to their weapons. They fire off a barrage of questions to confirm the facts they’ve received from dispatch. You’re not sure you’re answering adequately; you’re afraid, and you’re distracted by the officers’ authoritative presence, their weapons.
They thank you and conclude the encounter abruptly, signalling with their tone and body language that the conversation is over. They walk past you to your loved one, and your anxiety spikes. Will these officers be able to help? Will your loved one be safe with them? Are these cops some of the “good ones?” History has taught you that the individuals mandated to protect safety don’t always do so. When they fail, the consequences are traumatic and sometimes deadly.
So begins an essay by Haughton and Bromberg.
They suggest that Canadian cities should look internationally for alternative models:
“From Stockholm, Sweden’s Mental Health Ambulance to Eugene, Oregon’s CAHOOTS program; from Denver, Colorado’s STAR teams to North Yorkshire’s mental health triage nurses; from the Bay Area’s youth crisis services, to Austin, Texas’s EMCOT teams, to crisis teams under construction in Oakland, Portland, San Francisco, Albuquerque, and New York City, cities are recognizing that mental health crisis is a health crisis, not a crime, and should be treated accordingly.”
Ultimately, they envision a new service:
“Toronto must create a fourth emergency service, led by mental health clinicians and peer workers from the communities they serve, to respond to mental health crises. This team must be incorporated into municipal services and accessible either through 911 or through an easy-to-recall number like 811. It must be available 24/7, with response times equivalent to police and ambulance response times.”
A few thoughts:
- This is a well-argued essay.
- There have been tragic outcomes in recent months – but problems have existed for years. Would more police training be appropriate? Are the authors right in calling for a different approach altogether?
- An update: Toronto City Council voted to study the concept.
The essay can be found here:
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments