From the Editor
“So to put it simply, forcing people to choose is not always wise, and remaining neutral is not always possible.” University of Chicago economist Richard H. Thaler and Harvard Law School Professor Cass R. Sunstein write this comment in their widely-read book Nudge: Improving Decisions about Health, Wealth and Happiness. They argue that people could be nudged in a certain direction, improving outcomes. Among the book’s fans: former UK Prime Minister David Cameron and former US President Barack Obama.
Thaler and Sunstein write about shaping basic decisions, like encouraging people to choose among their company’s pension plans. Retirement planning can significantly help people with their finances in their twilight years. But what about substance use? The stakes seem higher: smoking cessation can prevent major health problems long before retirement.
This week, we look at a new paper by University of Pennsylvania Perelman School of Medicine’s Dr. Scott D. Halpern and his co-authors. Published in The New England Journal of Medicine, they consider smoking cessation and find “financial incentives added to free cessation aids resulted in a higher rate of sustained smoking abstinence than free cessation aids alone…”
 Nudging people to butt out?
Nudging people to butt out?
In this week’s Reading, we consider the paper and its implications. (There is, however, no financial incentive offered here.)
DG
“A Pragmatic Trial of E-Cigarettes, Incentives, and Drugs for Smoking Cessation”
Scott D. Halpern, Michael O. Harhay, Kathryn Saulsgiver, Christine Brophy, Andrea B. Troxel, Kevin G. Volpp
The New England Journal of Medicine, 14 June 2018 (Open Access)
https://www.nejm.org/doi/full/10.1056/NEJMsa1715757
Most large U.S. companies offer smoking-cessation programs for their employees, and nearly half of those companies offer financial incentives for employees who successfully stop smoking. These benefit designs are motivated by evidence that smoking remains the leading cause of preventable illness and death in the United States and that employees who smoke cost the companies several thousand dollars more per year than nonsmokers. However, the benefits offered by workplace smoking-cessation programs vary considerably, and there is limited evidence regarding the absolute or comparative effectiveness of these programs.
Two previous randomized, controlled trials involving employees who were interested in quitting smoking — one that included 878 employees of General Electric and one that included 2538 employees of CVS — showed that financial-incentive programs of approximately $800 tripled the rates of abstinence through 6 months as compared with approaches that offered only free access to behavioral-modification programs and informational resources. However, some key questions remained unanswered: How successful would workplace smoking-cessation programs be among all people to whom they were offered (rather than only among smokers who were interested in quitting, as tested in previous trials)? How effective would incentives be when added to free nicotine-replacement therapy and pharmacotherapy (i.e., bupropion or varenicline)? And how effective would free electronic cigarettes (e-cigarettes) or free conventional cessation aids be when added to provision of information on smoking cessation and access to motivational text-messaging programs?
A fourth unanswered question was raised by the CVS trial, in which an $800 reward was compared with an $800 ‘deposit contract,’ in which participants deposited $150 that was matched with $650, such that up to $800 was forfeited if the participant did not stop smoking. Among smokers who would have accepted either the reward or deposit contract, the deposit program was more than twice as efficacious as the reward program, probably because it leverages loss aversion. However, because only 13.7% of the participants who were offered deposit contracts chose to participate, the overall effectiveness of this approach was lower than that with standard financial rewards. Might deposit contracts that are funded in advance without participant contributions, but from which money is removed if abstinence milestones are not met, achieve higher engagement and smoking-cessation rates by leveraging loss aversion among a broader pool of participants? We conducted the current trial to address these four key questions.
 Scott D. Halpern
Scott D. Halpern
So begins a paper by Halpern et al.
Here’s what they did:
- “We conducted a randomized, controlled trial that compared five approaches to smoking cessation: usual care and four interventions designed to promote sustained smoking abstinence.”
- Participants were employees and their spouses at 54 companies, at least 18 years old, and had reported smoking on a health risk assessment within the previous year.
- The usual care included information on the benefits of smoking cessation and a motivational text-messaging service.Participants in the intervention groups received the usual care, and one of four programs: “free cessation aids, which included all forms of nicotine-replacement therapy, bupropion or varenicline, and – for participants who reported lack of success with initial standard therapy – free NJOY e-cigarettes (including battery sticks, a USB charger, and up to 20 chambers with 1.0 to 1.5% nicotine per week in participants’ chosen flavors); free e-cigarettes without the requirement that standard therapies had first been tried; a reward incentive worth $600 for sustained smoking abstinence, plus all options in the free cessation aids group; or a deposit account worth $600, redeemable by participants who become abstinent, plus all free cessation aids.”
- The primary outcome was sustained smoking abstinence for 6 months (after the target quit date).
- They also considered the “engaged” cohort – who were defined as “all participants in the intention-to-treat population who accessed the trial website at least once.”
Here’s what they found:
- 6,131 employees from 54 companies were invited to enroll with 125 (2%) opting out; 6,006 employees were thus randomized.
- Demographically, the median age was in the mid-40s; people had high school or better in terms of education; participants’ gender was slightly more female than male. The engaged cohort (1191 participants or 19.8%) tended to be more educated and more likely to use e-cigarettes.
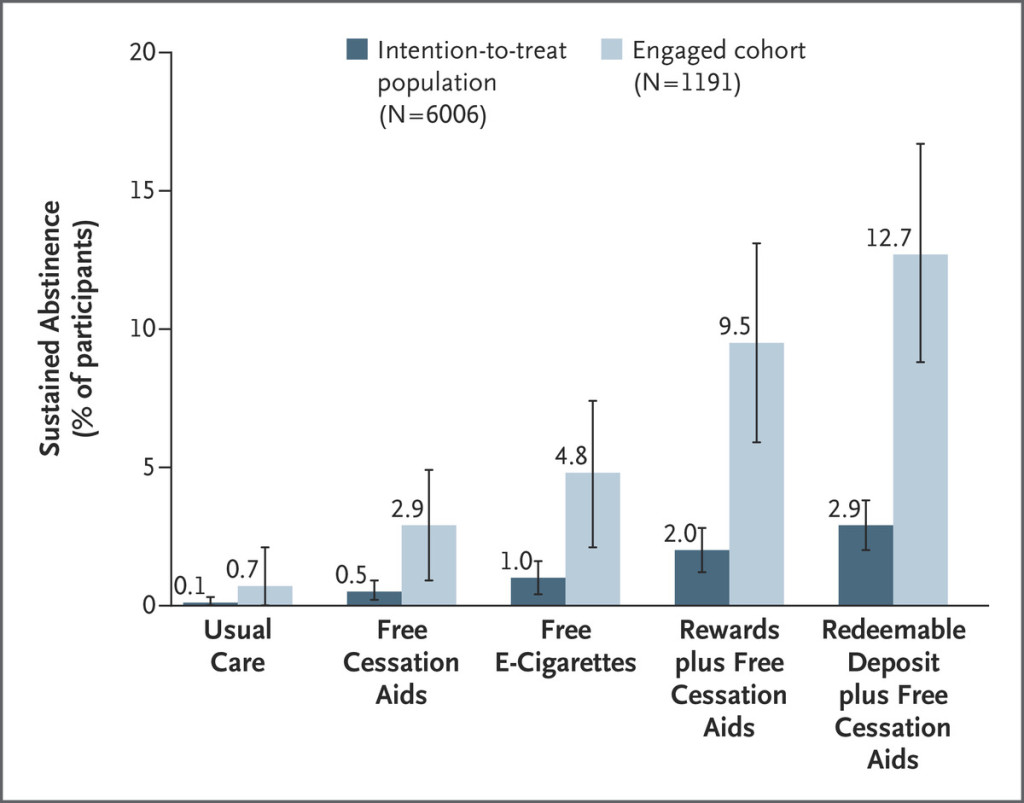
- Among all participants, sustained abstinence rates through 6 months were 0.1% in the usual-care group, 0.5% in the free cessation aids group, 1.0% in the free e-cigarettes group, 2.0% in the rewards group, and 2.9% in the redeemable deposit group. Of note: deposits were superior to free cessation aids (odds ratio, 5.77), rewards were superior to free cessation aids (odds ratio, 3.95), and redeemable deposits were superior to free e-cigarettes (odds ratio, 2.95).
- Among participants in the engaged cohort, the rate of sustained smoking abstinence through 6 months after the target quit date was 0.7% in the usual-care group, 2.9% in the free cessation aids group, 4.8% in the free e-cigarettes group, 9.5% in the rewards group, and 12.7% in the redeemable deposit group.
- Of note in the engaged cohort: redeemable deposits were superior to free cessation aids (odds ratio, 4.85) and to free e-cigarettes (odds ratio, 2.93), and rewards were superior to free cessation aids (odds ratio, 3.47).
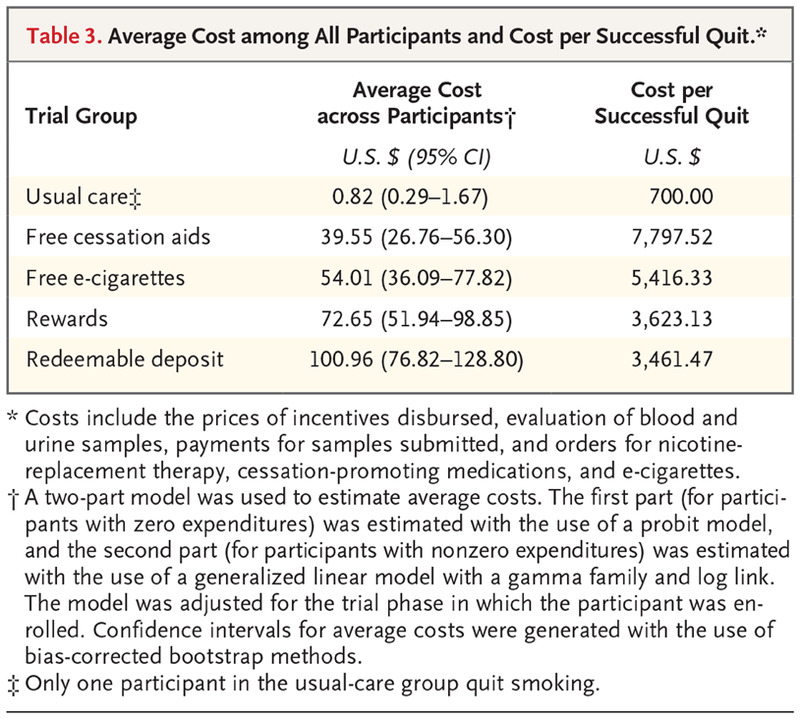
- “Average costs per participant assigned to each intervention were lowest in the usual-care group ($0.82) and highest in the redeemable deposit group ($100.96). The overall cost of each program per participant who was abstinent for 6 months was lower in the rewards and redeemable deposit groups than in the free e-cigarettes or free cessation aids groups…”
The authors make a few points:
On workplace smoking-cessation programs –
By using opt-out consent, we found that the quit rates that are likely to be achieved with workplace smoking-cessation programs were lower than would be surmised on the basis of previous workplace studies that measured cessation among smokers who were motivated to quit.Specifically, the most effective intervention in the current trial produced a 6-month sustained abstinence rate of only 2.9% among all smokers to whom the program was offered.
On the usual care vs. e-cigarettes –
Among smokers who had access to information about smoking cessation and the opportunity to sign up for motivational text messages, neither the additional offer of free e-cigarettes nor the additional offer of free first-line cessation aids (plus e-cigarettes if those failed) significantly improved rates of smoking abstinence. The lack of effectiveness of free cessation aids is important, because this practice is a cornerstone of many employers’ wellness programs.
On financial incentives –
This trial showed that financial incentives promoted smoking cessation even when free pharmacologic cessation aids and nicotine-replacement therapies were routinely available. These results, considered alongside those from previous trials, suggest that incentives at least triple cessation rates regardless of whether free cessation aids are offered concomitantly.
A few thoughts:
- This is a good study.
- There is much to like here. This is a well-designed study that doesn’t just consider people interested in quitting, but looks at all smokers. Other features of the study worth noting: the large number of people involved, and the study used a PRECIS-2 design.
- It’s difficult to get people to quit cigarettes. The usual care resulted in a quit rate of 0.1%. Ouch. People in the rewards group did significantly better – but still had a very low quit rate.
- The authors also considered costs – which is the way we ought to think about public-health interventions. From the paper:
- Remember that the study considered those eligible for employer-sponsored plans. So, demographically, people tended to be more educated and more female (and, yes, employed). That’s a contrast from the reality of smoking in a country like Canada, where the overall rate is falling, but not so much among those of lower socioeconomic status and those with mental illness. Here’s a Statistics Canada summary of the overall trend:
That’s not a criticism of Halpern et al., but an invitation to see their work in a larger context.
University of Toronto’s Dr. Peter Selby, head of CAMH’s Nicotine Dependence Clinic, is widely published in the area of smoking cessation. He notes:
This paper and the body of work done by this group of authors on workplace-based incentives should not change clinical practice away from evidence-based medicines and counselling for those addicted to cigarettes. It also doesn’t shed light on the effectiveness of e-cigarettes. Although participants were eligible for smoking cessation aids, actual use was not measured and appears to be low even in the engaged sample. Moreover, incentives need to be of sufficient amount and salient to the individual participant which certainly wasn’t the case in this study.
Workplace incentive studies generally do not include those with mental illness or on disability. I believe it would be unethical to blindly apply these findings to our patients, especially to those on already meagre social assistance. Due to the stigma of substance use disorders, it would likely be implemented as a loss-aversion program where income would be withheld if the person smoked. This thinking fails to appreciate the ‘use despite harm’ criteria of substance use disorders and that our patients with compromised executive function already use funds to buy cigarettes instead of food. Worse still, many of my patients report picking up butts off the street to smoke. Making cost-free medications and CBT for our patients easily accessible in every mental health program will have an impact on their lives. As a clinician, we need to remember that one of every two smokers will die prematurely from a tobacco related disease. Helping them quit, saves lives.
- Health care poses many challenges for behavioural economics. This paper considered an effort to “nudge” patients. Nudging providers have produced mixed results. In a CMAJ paper by Rudoler et al., the authors considered whether financial incentives might encourage physicians to care for patients after hospitalization or suicide attempts. They didn’t. (A past Reading considered this paper, which you can find here: http://davidgratzer.com/reading-of-the-week/reading-of-the-week-better-pay-better-service-the-cmaj-paper-on-pay-for-performance-in-psychiatry-also-a-fathers-memory/.)
(Many thanks to Dr. Selby for his emails about this paper, helping me understand it better.)
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments