From the Editor
“Bobby became my intern, and I was his senior resident. It was a role I cherished, and I tried to teach him all I could about caring for multiple sick patients simultaneously and navigating the systems, personalities, and politics of a large Manhattan hospital.”
Dr. Richard E. Leiter (of Harvard University) writes these words in a New England Journal of Medicine paper, this week’s first selection. He discusses loss – specifically, the death by suicide of the junior resident he was working with. On Twitter, Dr. Leiter commented that it took him six years to write about this death. Reading over the paper, we can understand why; the essay is deeply personal and moving. It also seeks to be constructive: Dr. Leiter calls for change. “Seeking to improve the lives of others shouldn’t cost our trainees their own.”

Of course, the NEJM article isn’t just about Bobby; it touches on the culture of medicine. Suicide, while always tragic, is rare in health care; untreated depression and substance problems are too common. In the second selection this week, we consider a paper recently published in JAMA Internal Medicine. Dr. Erene Stergiopoulos (of the University of Toronto) and her co-authors note the mixed message of medical education: at once encouraging “wellness” but also criticizing time away. “Stigma surrounding depression is deeply embedded in medicine.” Importantly, Dr. Stergiopoulos and her co-authors makes three practical suggestions.
* * *
On a pivot –
Since 2014, the Reading of the Week (ROTW) has been providing summaries and commentary on the latest in the psychiatric literature. Two years ago, we conducted a short survey to get your feedback. We are hoping to get more feedback to improve the Readings further.
We would invite you to join one of our online focus groups to hear your opinions and suggestions for improvement. If you are interested in participating, please email smit.mistry@camh.ca by April 12 with your preferred time slots from the following options – psychiatrists: April 21 at 4 pm or April 22 at 4 pm; residents: April 28 at 4 pm and April 29 at 4 pm. (Note: all times are in EST.) Time commitment: under an hour. If the above time slots do not work for you, please email Smit to arrange an interview time at your convenience, ideally between April 21 and April 30, 2021.
DG
Selection 1: “My Intern”
Richard E. Leiter
The New England Journal of Medicine, 18 March 2021

‘Bobby hasn’t come in yet today,’ one of my chief residents told me. ‘He isn’t picking up his phone or answering his pager. Could you go and check on him?’
I was in my final year of my internal medicine residency and was on a 6-week rotation as the assistant chief resident. In this role, I organized educational sessions for the residents and medical students and helped with administrative tasks. Most important, I learned how to support other residents and respond to their needs, which is what much of my job as chief resident would entail the next year.
Bobby was an intern in our program, and he and I had worked on a team together in early July. Bobby became my intern, and I was his senior resident. It was a role I cherished, and I tried to teach him all I could about caring for multiple sick patients simultaneously and navigating the systems, personalities, and politics of a large Manhattan hospital. We stayed late as we struggled to place an ultrasound-guided IV into the arm of a patient whose veins were shot from years of dialysis. Perched side by side on a windowsill, we nearly missed morning rounds as we listened to a dying patient recount his journey from India to the United States. By the end of our long, busy month together, I was proud of the doctor Bobby had already become.
So begins a paper by Dr. Richard E. Leiter.
Concerned, they go to Bobby’s apartment: “We soon discovered the incomprehensible reality: Bobby had jumped out his window. The usual din of the Manhattan street below was eerily quiet. Cecil’s Internal Medicine lay open on his tiny kitchen table, the pages gently flapping in the breeze from the open window.”
He notes the impact of the loss. “The sudden death of a colleague would shake any workplace; in a medical training program where the boundary between the personal and the professional blurred into near nonexistence, its effect was seismic. When Bobby died, we asked the same questions of ourselves that others do when a close friend dies by suicide: What could we have done to prevent it? What had we missed? But we also had a different set of questions: Had something happened to our colleague in the hospital the night before he died?”
The paper talks about the loss. Dr. Leiter goes to the funeral in another state and talks to his family. “‘Bobby told me you were the perfect resident; he wanted to be just like you.’ Though she meant it as high praise, her comment left me rattled. I couldn’t escape thoughts that my expectations were too high or that I should have picked up on something wrong while I was working so closely with him.”
“I threw myself deeper and deeper into my job, hoping that working to heal my patients’ suffering would shield me from my own. I kept my head down on my way into the hospital each morning, lest I catch a glimpse of Bobby’s window. Predictably, this strategy was unsustainable. Evaluating a new patient in the ED, I found myself in the same corner where I had watched my colleagues work on Bobby. I couldn’t muster the wherewithal to inhabit my role as a physician while also containing my terrifying memories. After rounds, I sobbed in my chief resident’s office. I saw Bobby’s death as a sign of my failure. I had failed as a resident. I had failed as a teacher. Bobby was my intern and I had failed him.”
“Thankfully, I received the psychiatric services I so desperately needed. I still have a scar, but it’s well healed.”
A few thoughts:
- This is a beautiful essay.
- Dr. Leiter touches on the uniqueness of our jobs and training: “On Saturday nights, other people my age discovered new bands and ate at trendy new restaurants; I fought with the electronic medical record to input orders for laxatives and stood in line to perform chest compressions on a dying mother of two young children.”
- It’s also true that there is a cultural component. Doctors don’t get sick, we like to believe, and we certainly don’t get sick with mental illness – except, of course, that we do. Dr. David Goldbloom notes: “it is a sobering reminder that the white coat is not Kevlar against the illnesses we treat, and our professional culture still has a long way to go in recognizing, accepting and supporting that we get sick, too.”
The full NEJM paper can be found here:
https://www.nejm.org/doi/full/10.1056/NEJMp2004154
Selection 2: “Cultural Barriers to Help-Seeking in Medical Education”
Erene Stergiopoulos, Ligia Fragoso, Lisa M. Meeks
JAMA Internal Medicine, 28 December 2020
![]()
Depressive symptoms are common in medical trainees. In medical school and residency, studies estimate that approximately one-quarter of trainees may have depression or depressive symptoms, whereas only approximately one-sixth of such trainees seek mental health treatment (psychotherapy or pharmacotherapy). The disconnect between depressive symptoms and help-seeking is disconcerting.
In this article, we consider the well-established literature about medical students and residents with depression and depressive symptoms to understand the cultural barriers to help-seeking and to inform recommendations for attitudinal and structural changes. Depressive symptoms pose many overlapping challenges for trainees, including burnout, anxiety, and other common forms of distress that affect well-being and performance. Therefore, although our recommendations use depression as a starting point, they address barriers inherent in the overarching medical learning environment and the numerous challenges to the well-being of trainees.
So begins a paper by Stergiopoulos et al.
They note the contraction in medicine. “Despite a stated commitment to learner well-being, the culture of medicine continues to foster maladaptive perfectionism and silence for those with depression. Although medical schools and residency programs have invested increasingly in wellness initiatives to support individual resilience, the learning environment itself is often the most substantial driver of distress. Learners thus encounter mixed messages in their training; programs claim to value their well-being yet promote institutional policies and norms that reward self-sacrifice and increased productivity. Too often, help-seeking and time off are perceived as signs of weakness or poor work ethic. Indeed, trainees report the most substantial barrier to their well-being is the lack of time or flexibility to attend to their physical and mental health needs. Taken together, these experiences contribute to a learning environment that explicitly promotes self-care yet implicitly labels these actions as incompatible with the demands of medical practice.”
They offer three practical suggestions:
Create Opt-Out Counseling Programs
“Programs should consider an opt-out system whereby all trainees have access to at least 3 confidential sessions with a therapist during the transitions to medical school and residency, which are associated with increased distress. Opt-out mental health sessions during medical training normalize help-seeking and provide space to process personal and professional experiences.”
Encourage Physician Role Models to Share Their Mental Health Experiences
“Programs can provide safe platforms for faculty to share their experiences – for example, through panel discussions or faculty-led small group sessions focused on physician and trainee mental health. Ideally, such activities should also provide information about the institutional and private mental health services that are available.”
Resist the Default to Leaves of Absence for Mental Health Concerns
“Before endorsing leave of absence, medical schools and residency programs should consider and implement program modifications and accommodations that allow trainees to continue and to thrive. For example, learners may benefit from protected time for mental health appointments, adjustments in call schedules, and modified schedules….”
A few thoughts:
- This is a good paper.
- The authors make strong recommendations. For the record, I think that the second suggestion is particularly important.
- They also offer evidence to support the recommendations. For example, a pilot of the “opt-out counseling” showed robust results: “Evaluation of the initiative indicated high participation, with 38 of 41 postgraduate year 1 and 2 residents (93%) engaging in the assessment in the first year and 100% of the postgraduate year 1 residents participating in year 2 of their training.”
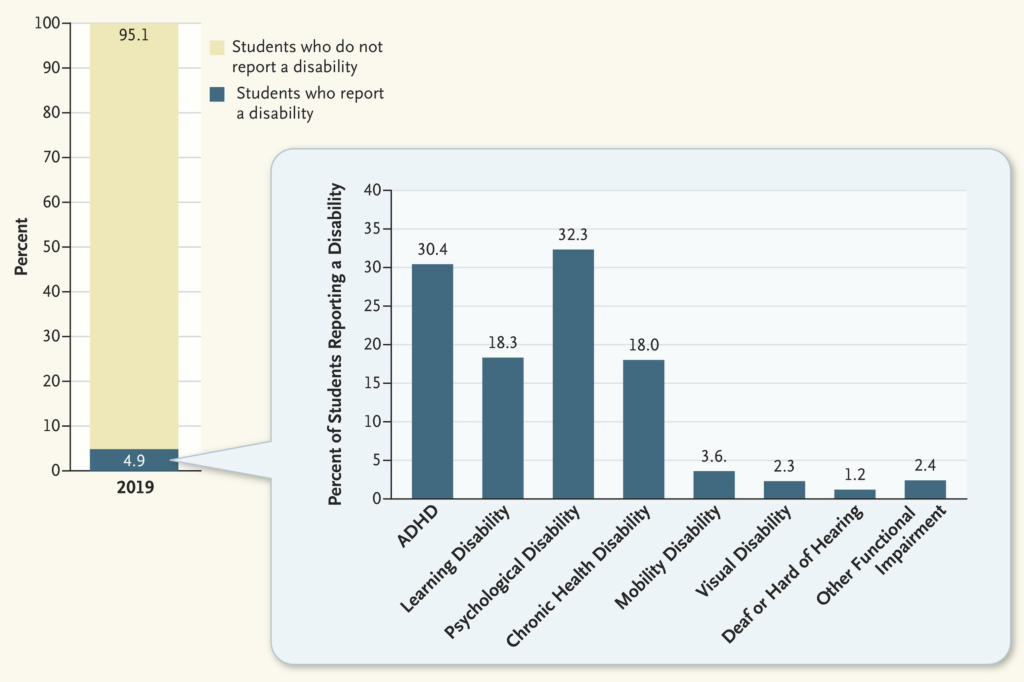
- How big a problem do we have? In a recent NEJM paper, Dr. Omar S. Haque (of Harvard University) and his co-authors write: “Despite calls for greater awareness of high rates of depression and suicide among physicians, estimates suggest that only about 1% of medical students with major depressive disorder disclose it as a disability.” The paper goes into more detail.
That paper can be found here: https://www.nejm.org/doi/full/10.1056/NEJMp2031013
The full JAMA Internal Medicine paper can be found here:
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2774563
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments