From the Editor
After a break, the Readings are back. In the coming weeks, we will consider important papers on depression treatment, cannabis, help for the homeless, and more.
This week, there are two selections.
In the first selection, we consider the new Globe and Mail essay by reporter Erin Anderssen on the supply (or the lack of supply) of psychiatrists across Canada. This essay does a sparkling job of pulling together stories and reports, and includes an overview of the literature. It paints a familiar, if unsettling, picture of need unmatched by availability, and includes interviews and original data analysis.
She writes: “The modern psychiatrist can’t be everywhere. So they should be where Canadians need them most.”
We summarize the essay and some of the larger questions raised.
 Erin Anderssen
Erin Anderssen
In the second selection, the Vrije Universiteit Amsterdam’s Pim Cuijpers writes about depression and treatment. Thinking about successful care, he asks a simple question: “When patients seek treatment, is a reduction of depressive symptoms really what they want, or do patients have other goals as well?”
DG
“Half of Canadians have too few local psychiatrists, or none at all. How can we mend the mental-health gap?”
Erin Anderssen
The Globe and Mail, 18 January 2020
In London, Ont., a 20-year-old man waits a year to see a psychiatrist after he is hospitalized for suicidal behaviour.
In Prince Edward Island, even the most serious patients on the provincial triage list are told in November they will wait at least six months to see a psychiatrist.
When the only staff psychiatrist at Lake of the Woods District Hospital in Kenora, Ont. decides to move, the community is left begging for help from Thunder Bay, 500 kilometres away, where psychiatrists there already scramble to cover an area roughly the size of France.
Across the country, Canadians tell similar stories of too few psychiatrists in places with too many patients in the queue. The results of the critical shortage: jam-packed emergency departments, long wait lists, stressed-out families, and burned-out doctors.
So begins a front-page Globe article on mental health services in Canada.
The essay is challenging to summarize. It combines personal anecdotes with substantive public policy discussions. And it points in one clear direction: Anderssen notes the dearth of access to psychiatrists – and the incredible variation by geography.
Brampton, Ont., one of the fastest-growing – and youngest – municipalities in the country, has about one psychiatrist for every 24,000 people, one of the worst ratios in Ontario. By comparison, Toronto, just 40 kilometres away, has a ratio of one psychiatrist for every 2,754 people.
The article reviews the literature, drawing heavily on the work of Dr. Paul Kurdyak, a psychiatrist affiliated with CAMH and the University of Toronto:
- “In Toronto and Ottawa, 40 percent of full-time clinicians saw fewer than 100 patients a year…Ten percent saw fewer than 40 patients.”
- “The patients seen by those smaller-volume psychiatrists were more likely to live in higher-income neighborhoods, and less likely to have been previously hospitalized for psychiatric issues.”
- “40 per cent of Ontario youth discharged after an emergency department visit for their first psychotic episode received no outpatient mental health care for 30 days – despite research showing that follow-up is a key factor in preventing re-hospitalization.”
- “A 2017 paper found that the majority of people treated in an Ontario emergency department after a suicide attempt were not seen by a psychiatrist within six months…”
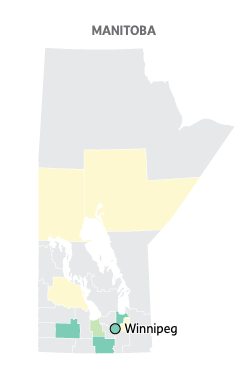 Psychiatrist supply in Manitoba: vastly better in the cities (source: Globe)
Psychiatrist supply in Manitoba: vastly better in the cities (source: Globe)
What are the implications for mental health care reform?
Philip Klassen, vice president of medical services at Ontario Shores Centre for Mental Health Sciences, comments: “We have a long and cherished history that allows health professionals to do more or less what they want, in terms of who they see and the interventions they provide. At first blush, you can say we lack resources. But I think the first order of business is to ask, what are we doing with our resources?”
The essay also looks at some ideas for reform:
- Central registries that would steer patients to psychiatrists. Quebec has experimented with the idea (regional centralized registries), and they are used for other specialty service.
- Collaborative care teams with psychiatrists, who would provide both rapid consults and follow-up care, “ideally supported by psychiatric nurses, psychologists and social workers.”
- Innovative approaches, like treating patients in groups as part of the outpatient mental health services. St. Paul’s Hospital experimented with this approach, with 15,000 patient visits in 2016, as opposed to 400 in 2014 with the more conventional one-on-one follow ups.
Anderssen writes further about other ideas, like the better use of technology (telepsychiatry); she also mentions some low-tech solutions (e.g., dropping boundary lines in hospital service areas). And she acknowledges the challenges of making changes; for the record, the St. Paul’s Hospital project fizzled out.
Ultimately, a system upgrade would make the psychiatrist’s job more efficient and more focused. As advocates for change such as Dr. Kurdyak suggest, that means moving out of solo practice and into spaces with other doctors and mental health professions, embracing technology to spread their clinical reach, and concentrating on the toughest cases they are best trained to handle.
A few thoughts:
- This is an important essay.
- Anderssen adds to the debate, in part by offering clear data. Readers may or may not agree with the policy prescriptions, but the description of the national problem is outstanding and lucid.
- Some of the stories are tough to read. As an example, Anderssen speaks with a family doctor in Vancouver. When a local psychiatrist retires, she tries to find a replacement to help her with six challenging cases. “Honestly, we don’t even bother [looking] anymore…” Instead, the patients are routinely sent to the ED. Ouch.
A few years ago, Goldner et al. considered how many Vancouver psychiatrists could see a patient with major depressive disorder in a timely manner. Of the 230 psychiatrists contacted, six offered an appointment within 4.5 weeks.
That Canadian Journal of Psychiatry paper can be found here:
https://journals.sagepub.com/doi/abs/10.1177/070674371105600805
- What’s the way forward? Anderssen mentions several ideas. Are they persuasive? Anderssen envisions a different role for psychiatrists. How do we, as clinicians, feel about this?
- Do you have thoughts on this essay? Ideas for mental health reform? As always, the Reading of the Week invites letters to the editor.
- The essay focuses on access and the agenda of patients (and their families) to get better access. But what is the patient agenda in terms of outcomes? The next selection asks this question.
“Measuring success in the treatment of depression: what is most important to patients?”
Pim Cuijpers
Expert Review of Neurotherapeutics, 14 January 2020
https://www.tandfonline.com/doi/full/10.1080/14737175.2020.1712807
In the past decades, hundreds of randomized trials have shown that pharmacotherapies, psychotherapies, and several other therapies are effective in the treatment of depression. These trials typically focus on the effects of treatments on depressive symptoms, response, and remission. But when patients seek treatment, is a reduction of depressive symptoms really what they want, or do patients have other goals as well?
This is a highly relevant question, not only because there is a growing recognition of the importance of patient-defined outcomes and the need to involve people with lived experience in research and clinical practice…
 Pim Cuijpers
Pim Cuijpers
Cuijpers, a prolific Dutch researcher, writes about two aspects of patients and outcomes.
Patient-defined outcomes in mental health treatment
“This research shows that patients find symptom reduction a very important goal of therapy, but it is certainly not the only goal.” He notes that patients want “to be able to go back to work, have a more fulfilling life, solve conflicts with partners…”
He argues that some attempts have been made to produce measureable outcomes, like the Target Complaints, which dates back to the 1960s: “the patient describes three target complaints in a clinical interview, and for each of these complaints both the therapist and patient rate how much the problem is bothering the patient. After treatment, both the therapist and patient again rate these problems, but now indicate on a five-point scale how much the problem has improved.”
That said, “What the problems are that patients consider important has not been examined extensively, and is mostly limited to small studies in selective patient samples…”
The effects of treatment of depression on quality of life and other outcomes
“There is a considerable literature showing that treatment of depression not only affects depression, but many other outcomes.” He writes: “quality of life, social functioning, anxiety, hopelessness, dysfunctional thinking, and social support.”
“These meta-analyses find a strong correlation between the effects of treatments on depression and those on the secondary outcomes. Although this cannot be considered as causal evidence, it suggests that successful treatment of depression also has significant effects on these other areas of life. Although patient-defined outcomes have not been examined extensively, this research makes clear that treatment of depression goes beyond effects on depressive symptomatology, and also positively affects other relevant areas of life.”
He goes on to argue for more consideration in this area.
It is time that we start recognizing these patient-defined goals more than has been done until now, not only because patients deserve more recognition of their needs, but also because depressive disorders are not the clearly defined entities as our diagnostic systems suggest. In order to understand depressive disorders and their treatment better, we have to take a broader perspective, and take the patient perspective into consideration in our research.
A few thoughts:
- This is an excellent paper.
- Cuijpers is prolific, and has written many important papers on depression. (Next week’s Reading will include consideration of his new network meta-analysis from World Psychiatry.) Still he recognizes the need for studies to tie better into the needs and agendas of our patients.
- On this topic, The Lancet Psychiatry has just published a good editorial, “Measuring success: the problem with primary outcomes.”
The editors write:
As in any clinical field, there may be disagreement about the choice of outcomes, and the clinical experience and personal preferences of investigators no doubt play a role in the selection of a primary outcome. Studies also need to be comparable with previous work. Using the same scales facilitates these direct comparisons and the use of findings in future meta-analyses. Other concerns, like obtaining funding and future regulatory approval for a tested treatment, might also influence which measurement scales are preferred by investigators when planning an RCT. Conspicuously absent from these considerations – that mainly affect and are dictated by researchers, editors, and government officials – is the question of whether the primary outcomes chosen in RCTs for psychiatric disorders capture what is most important to a patient or service user. Does a statistically significant change in the Hamilton Rating Scale for Depression, the Montgomery-Åsberg Depression Rating Scale, or the Beck Depression Inventory score actually represent a meaningful improvement in the life of someone living with depression?
That journal has just announced that people with lived experience will now serve on the journal’s editorial board.
The editorial can be found here:
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(19)30483-3/fulltext
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
January 23, 2020 at 6:16 pm
Hi David:
I read that article in the Globe last weekend and have a few thoughts.
I am general adult psychiatrist working in oncology (inpt and outpt) and complex care units (pts in enhanced LTC units with TBI, dementia +, Huntington’s etc).
1. These programs want me to act as solo practitioner – overall they don’t want to pay for a psych nurse to work with me. Because I bill AHS and RN would require funding. So in oncology no nurse is provided. No assistance whatsoever provided. Almost no admin. For complex care – the managers say the RN is only ‘supposed to do new consults’ and I’m on my own for follow ups. In practice we do both. But it’s a constant fight that gets brought up over and over again. Complex care really does not lend itself to a one time assessment.
Also with new and more difficult EMRs I find my productivity has decreased. Definitely not improved and I take more time on the computer and less time actually providing patient care. Some of admins responsibilities it seems to me have been downstreamed to the MDs – again not cost efficient but the clinics frankly don’t mind because they have reduced their admin cost and don’t pay the MDs. We are all FFS.
And then finally I do think pay for new pts versus follow ups needs to change and complex vs non complex needs to change. There are very few incentives to work with more challenging groups. Very few incentives to book people who no show – up to half the time – with no compensation for these empty blocks of time.
Just some thoughts
Thank you for your writing
January 23, 2020 at 8:39 pm
It’s a challenge, isn’t it, to bring these papers into the larger picture of how we care for the vast numbers of people suffering in our contemporary society.
The answer is that psychiatrists, on their own, are not an answer, and psychiatric consults, without access to trauma-informed individual and group psychotherapy, social work, attention to housing and nutrition and community will generally create more problems than it solves.
The vast majority of our patients are suffering from “mental” illnesses that are not treatable (or only marginally treatable) by medications, or short-term therapies, and many are secondary to social breakdown, poverty and loneliness.
As the second paper notes, patients are seeking a wider range of outcomes, and we know these outcomes are associated with return to health and productivity, while there is no such relationship if we just look at symptom reduction.
In fact, if we base our system on CBT, medications and symptom reduction, we will continue to see rising rates of violence, broken families and broken lives as well as climbing rates of suicide and emergency department admissions.
Recruiting older psychiatrists who are now practicing psychoanalysis or long-term psychotherapy to quickly assess and medicate acute patients will only add to moral injury; this is not where the solution lies.
Instead, we need a system that is first and foremost trauma-informed and that in doing so, actually cares for its providers and those in their care, and a system that holds each patient along the often long road of recovery.
We seem to know all of this, and to forget it as often as we re-learn it. Which is not to say that the challenge of creating a truly effective healthcare system that does not separate mind from body, that is free from the corruption and greed for power that permeates the mental health care culture, that instead serves a compassionate and honest vision – is not a daunting one.