From the Editor
Even with medications, the voices tormented him. My patient explained that his every move was commented on.
In avatar therapy, patients engage audiovisual representations of their voices, with the goal of reducing their influence. In the first selection, a new paper from Lancet Psychiatry, Lisa Charlotte Smith (of the University of Copenhagen) and her co-authors look at a new form of avatar therapy, with an immersive 3D experience. In this RCT, participants had enhanced usual care or the therapy; the severity of auditory hallucinations was then measured at 12 weeks. “Challenge-VRT showed short-term efficacy in reducing the severity of auditory verbal hallucinations in patients with schizophrenia, and the findings support further development and evaluation of immersive virtual reality-based therapies in this population.” We consider the paper and its implications.

In the second selection, Dr. Mark Ainsley Colijn (of the University of Calgary) writes about psychosis and rare genetic variation. In a Canadian Journal of Psychiatry paper – part of the new Clinician’s Corner series – he offers suggestions for antipsychotic meds. “When providing care for individuals with psychosis occurring on the background of rare genetic variation, psychiatrists should take the time to educate themselves accordingly to ensure the safe and rational prescribing of antipsychotic medications in this population.”
And in the third selection, from JAMA, Dr. Kumara Raja Sundar (of Kaiser Permanente Washington) comments on patients who use ChatGPT. The author, a family doctor, notes that many physicians can be paternalistic – but he urges against that instinct. “If patients are arming themselves with information to be heard, our task as clinicians is to meet them with recognition, not resistance. In doing so, we preserve what has always made medicine human: the willingness to share meaning, uncertainty, and hope, together.”
DG
Selection 1: “Immersive virtual reality-assisted therapy targeting persistent auditory verbal hallucinations in patients diagnosed with schizophrenia spectrum disorders in Denmark: the Challenge assessor-masked, randomised clinical trial”
Lisa Charlotte Smith, Ditte Lammers Vernal, Lise Sandvig Mariegaard, et al.
The Lancet Psychiatry, August 2025

Schizophrenia affects approximately 24 million people worldwide… Auditory verbal hallucinations, often referred to as hearing voices, are considered a primary symptom of schizophrenia and are prevalent in approximately 75% of this patient group. Although auditory verbal hallucinations are present across a range of psychiatric disorders, as well as among non-clinical voice-hearers without a need for care, the voices experienced by individuals with schizophrenia are often persistent, distressing, and characterised by critical or commanding content, making them a key therapeutic target in this group. Approximately one-third of people with psychosis have a suboptimal treatment response to antipsychotic medication and many report side-effects…
Cognitive behavioural therapy has shown some benefit in reducing auditory verbal hallucinations, although randomised controlled trials report only small to moderate effects, highlighting the need for improved methods. Relational psychotherapies have been developed based on findings that voice-hearers often personify the voices, and that hearing voices can be experienced as an opportunity for conversation and interaction. Among these approaches, some utilise technology to digitally embody the voice as an avatar displayed on either a 2-dimensional (D) screen or in 3D virtual reality. This approach facilitates a dialogue between the voice-hearer and the avatar representing a dominant voice, with the therapist assisting the voice-hearer in gaining confidence in standing up to the voice.
So begins a paper by Smith et al.
Here’s what they did:
- They conducted a randomized, assessor-masked, parallel-group superiority clinical trial.
- Patients with schizophrenia were recruited from outpatient psychiatric services across three Danish regions.
- Inclusion criteria included: age 18 years or older, auditory verbal hallucinations for at least 3 months, and insufficient symptom response to antipsychotic medication.
- Participants were randomly assigned with “allocation was concealed from outcome assessors.” Participants were assigned to either Challenge-VRT (seven weekly immersive virtual reality sessions plus two booster sessions) or a control intervention of enhanced treatment-as-usual, matched in frequency and duration. “Challenge-VRT is a manualised psychotherapeutic intervention comprising three phases. The first focuses on patients reclaiming power over the voice, the second on self-worth, and the final phase on recovery.”
- The primary outcome: reduction in the hallucination severity as measured by the Psychotic Symptoms Rating Scales-Auditory Hallucinations total score (PSYRATS-AH) at 12 weeks.
Here’s what they found
- 399 patients were referred for potential study inclusion; after exclusions, 271 participants were randomly assigned to Challenge-VRT (n=140) or enhanced treatment-as-usual (n=131).
- Demographics. Participants had a mean age of 32.83 years, and the majority were female (61%). No data was collected on ethnicity.
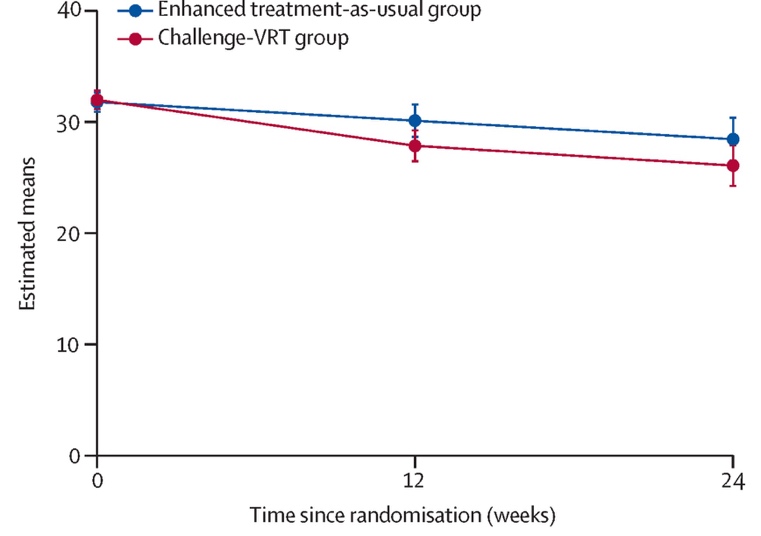
- Primary outcome. “At 12 weeks, Challenge-VRT significantly reduced auditory verbal hallucination severity compared with enhanced treatment-as-usual on the PSYRATS-AH (adjusted mean difference –2·26…).” See figure below.
- Secondary outcomes. “A significant reduction in PSYRATS-AH frequency was observed in the Challenge-VRT group at both 12 weeks (adjusted mean difference –0.84…) and 24 weeks (adjusted mean difference –0.86…).”
- Adverse events. The intervention was generally well tolerated. There were six serious events, including five who were hospitalized with exacerbation of their auditory hallucinations.
A few thoughts:
1. This is an interesting paper, attempting to address a common problem, and published in a major journal.
2. The main finding in a sentence: the intervention worked and produced a symptom reduction comparable to CBT – though it didn’t affect the overall social functioning of participants.
3. It’s difficult to debate the authors conclusion that further development and evaluation are worth pursuing.
4. Avatar therapy has caused a stir. The first big paper on the subject was published seven years ago (also in The Lancet Psychiatry); CNN did a story, as did others. The idea is cool and techie and creative. For those wanting to understand more about this therapy, the CNN piece is concise. You can find it here:
https://www.cnn.com/2017/11/23/health/avatar-therapy-schizophrenia-voices-study
5. But is avatar therapy practical? Results to date have shown short-term improvements, yes, but with positive effects fading quickly. In this new study, the authors laboured to engage patients: “29% of participants required additional time to manage anxiety before entering the virtual reality environment…” Indeed, anxiety was problematic. The experience was real. Was it ultimately too real for some patients?
6. It’s disappointing that the comparison was to enhanced treatment as usual, as opposed to 2D avatar therapy.
The full Lancet Psychiatry paper can be found here:
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(25)00161-0/abstract
Selection 2: “Rare Genetic Variation and Psychosis: Treatment Considerations for Psychiatrists”
Mark Ainsley Colijn
The Canadian Journal of Psychiatry, 21 July 2025 Online First

Numerous genetic disorders confer significant risk for the development of psychosis. Contemporary reviews on this topic have typically focused on describing ‘red flag’ features, outlining workup recommendations, and highlighting the importance of screening for comorbid medical issues. However, few if any articles have discussed the potential implications a genetic disorder diagnosis may have on antipsychotic selection. As such, this letter is intended to offer a practical framework for approaching the management of psychotic symptoms in individuals with rare genetic disorders. This is especially needed given the scarcity of formal treatment guidelines in this context. As genome/exome sequencing becomes more accessible at a reduced cost over the coming years, psychiatrists will presumably more frequently encounter patients with genetic disorder diagnoses, making this paper particularly timely. However, such testing is unlikely to become a routine part of clinical care for most individuals experiencing psychosis in the near term.
So begins a paper by Dr. Colijn.
He notes: “Rare genetic variation in and of itself does not contraindicate the use of antipsychotics, but many such conditions associated with psychosis also confer risk for neurodevelopmental abnormalities and various medical issues that may predispose to idiosyncratic side effects.” He adds: “As such, it is important to consider the physiological overlap between a given disorder’s possible comorbidities and the varying side effect profiles of different antipsychotics when providing care to individuals with genetic conditions.”
He makes several suggestions. Here, I focus on three.
Copy number variant syndromes
“As many copy number variant (CNV) syndromes (e.g., 22q11.2 deletion syndrome) confer risk for not only schizophrenia but also the development of seizures and congenital cardiac defects, antipsychotics that are less prone to lowering seizure threshold (e.g., aripiprazole, risperidone) and causing adverse cardiac effects (e.g., aripiprazole, cariprazine, lurasidone) may be preferable. Increased vigilance with respect to monitoring for signs of seizure activity and cardiac dysfunction before and during antipsychotic initiation/titration is also recommended. The prophylactic use of an anticonvulsant should additionally be considered when pursuing a clozapine trial.”
Wilson disease and Prader-Willi syndrome
“Similarly, given that Wilson disease and Prader-Willi syndrome are both associated with low bone mineral density/osteoporosis, partial dopamine 2 receptor agonists (aripiprazole, brexpiprazole, cariprazine) rather than antagonists may be a safer choice for such individuals, given their comparative effects on prolactin. As Prader-Willi syndrome is also associated with increased appetite and obesity, less metabolically problematic treatments should probably be favoured over quetiapine, olanzapine, and clozapine, all else being equal.”
22q11.2 deletion syndrome
“Another example involves the potential for early-onset parkinsonism in both 22q11.2 deletion syndrome and a variety of inborn errors of metabolism that can cause psychosis, such that antipsychotics with a lower likelihood of causing extrapyramidal symptoms (quetiapine and clozapine) may be better tolerated if motor dysfunction is present. Consideration should also be given to avoiding the use of (predominantly) renally excreted (e.g., paliperidone) and/or potentially nephrotoxic (e.g., lithium) psychiatric medications in patients with (or at high risk of developing) compromised kidney function due to congenital renal defects.”
“These examples highlight the need for psychiatrists to familiarize themselves with those genetic disorders that predispose to psychosis, when encountered clinically.”
He notes several online resources including the “online, peer-reviewed, journal-style, point of care resource, GeneReviews®” (https://www.ncbi.nlm.nih.gov/books/NBK1116) and OMIM which is a “useful website that focuses on genotype-phenotype correlations by collating relevant information from published reports” (https://www.omim.org).
A few thoughts:
1. This paper is concise and practical.
2. The key take-away message: “It is imperative that psychiatrists providing care for affected individuals become informed with respect to any potential medical comorbidities and make treatment decisions accordingly.” Thoughtful.
3. I look forward to highlighting more papers from the Clinician’s Corner series in the coming months.
The full Canadian Journal of Psychiatry paper can be found here:
https://journals.sagepub.com/doi/full/10.1177/07067437251339793
Selection 3: “When Patients Arrive With Answers”
Kumara Raja Sundar
JAMA, 24 July 2025

She came in for dizziness and described her symptoms with striking precision: ‘It’s not vertigo, more of a presyncope kind of feeling.’ Then she added, ‘I think a tilt table test might clarify what’s going on.’ Occasionally, a patient’s questions reveal a subtle fluency in medical jargon, suggesting they might have clinical training or at least have done a lot of reading. Following the breadcrumbs, I asked gently, ‘Do you work in health care?’ Usually, if a yes, the response is hesitant, perhaps concerned that their background might influence care. But this time, she looked down and quietly said that she had asked ChatGPT, and it mentioned tilt table testing.
So begins a paper by Dr. Sundar.
He argues that things have changed. “Patients arriving with researched information is not new. They have long brought newspaper clippings, internet search results, or notes from conversations with family. Potential solutions passed along in WhatsApp threads have at times been an integral part of my clinical conversations. Information seeking outside the health care setting has always been part of the landscape of care… But something about this moment feels different.”
He discusses his own exploration of AI. “I heard these tools were helpful, but I understood their appeal only after using them myself. Recent studies have bolstered this claim: large language models (LLMs) show surprising strength in reasoning and relational tone.” Though he feels that the comparison is “inherently unfair,” he also appreciates the enthusiasm of some patients. “After seeing it firsthand, my reaction was simple: ‘Man, I get why my patients like it.’”
Though much has changed, he observes that patients still come to see him – and that he, not ChatGPT, is on the hook for both liability and responsibility. “Clinicians remain the gatekeepers. In practice, this means navigating patient requests like a tilt-table test for intermittent dizziness – tests that are not unusual but may not be appropriate at a specific stage of care. I find myself explaining concepts like overdiagnosis, false-positives, or other risks of unnecessary testing. At best, the patient understands the ideas, which may not resonate when one is the person experiencing symptoms. At worst, I sound dismissive. There is no function that tells ChatGPT that clinicians lack routine access to tilt-table testing or that echocardiogram appointments are delayed due to staffing shortages. I have to carry those constraints into the examination room while still trying to preserve trust.”
He notes the paternalism of the medical profession. “The old line, ‘They probably WebMD’d it and think they have cancer,’ has morphed into the newer, just-as-dismissive line, ‘They probably ChatGPT’d it and are going to tell us what to order.’ It often reflects defensiveness from clinicians rather than genuine engagement and carries an implicit message: We still know best. It is an attitude that risks eroding the sacred and fragile trust between clinicians and patients. It reinforces the feeling that we are not ‘in it’ with our patients and are truly gatekeeping rather than partnering. Ironically, that is often why I hear patients turn to LLMs in the first place.”
He closes by noting the importance of relationships. “Patients may come with unrealistic expectations or cite recommendations that do not align with evidence-based guidelines or are impractical for a given resource setting. These moments are not new. We have long had to explain why a magnetic resonance imaging scan is not always needed for back pain or why antibiotics will not help a viral infection. We know the solution is not to shut these conversations down but to meet them with patience and curiosity. Medicine has always depended on relationships. What is changing is how those relationships begin and what patients bring to the table.”
A few thoughts:
1. This is a good paper – timely and relevant.
2. It’s amazing how much AI has changed medicine already.
3. He comments that AI “feels different.” It does – the conversational style of ChatGPT and other AI chatbots is a marked departure from a search on Google or a trip to the library stacks.
4. He makes other good points. The comment about relationships is particularly solid.
The full JAMA paper can be found here:
https://jamanetwork.com/journals/jama/fullarticle/2836827
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments