From the Editor
How do we connect with them?
With the worst of the third wave now behind us, we are beginning to look forward. But for some, the problems of the pandemic aren’t fading. They will continue to struggle with mental health problems.
Healthcare workers are particularly at risk. They are also, collectively, a group that is difficult to engage. In the first selection, we look at a new paper from The British Journal of Psychiatry. Dr. Doron Amsalem (of Columbia University) and his co-authors do a video intervention to increase treatment seeking. The resulting RCT is impressive. The authors write: “The high proportion of healthcare workers surveyed in this study who reported symptoms of probable generalised anxiety, depression and/or PTSD emphasises the need for intervention aimed at increasing treatment-seeking among US healthcare workers. A three-minute online social contact-based video intervention effectively increased self-reported treatment-seeking intentions among healthcare workers.”

In the second selection, Richard A. Brown (of the University of Texas at Austin) and his co-authors look at a new approach to an old problem: high smoking rates among people with severe mental illness. Focusing on inpatient hospitalizations, they design an intervention built on motivational interviewing. We consider their JAMA Psychiatry paper.
Is the term patient antiquated? Should we use other terms, like client or service user? In a BJPsych Bulletin paper, Dr. Stefan Priebe (of Queen Mary University of London) argues that we serve patients – and that words matter. “Mental healthcare is based on shared values and scientific evidence. Both require precise thinking, and precise thinking requires an exact and consistent terminology.”
DG
Selection 1: “Video intervention to increase treatment-seeking by healthcare workers during the COVID-19 pandemic: randomised controlled trial”
Doron Amsalem, Amit Lazarov, John C. Markowitz, et al.
The British Journal of Psychiatry, 5 May 2021 Online First

Healthcare workers are often reluctant to seek mental healthcare, with stigma regarding treatment being a profound obstacle. Stigma includes perceiving treatment-seeking as a weakness, anticipating negative attitudes of colleagues and supervisors, and fearing discrimination in career advancement. Stigma discourages treatment-seeking and has substantial consequences due to untreated mental health problems. Beyond increased risk of depression, suicide and other psychiatric problems, overstressed healthcare workers may report lower motivation, lose productivity and provide lower quality of care. Therefore, early detection and monitoring of healthcare workers’ mental health difficulties are crucial.
The COVID-19 pandemic has placed healthcare workers on the front line, exposing them to enormous stress and greater risk for anxiety, depression and post-traumatic stress disorder (PTSD). Healthcare workers already faced high risk for negative effects of chronic stress before the pandemic, risks now intensified by anxiety and fear. They grieve for patients who have died and feel guilt for not being able to save them. Healthcare workers fear getting sick themselves and experience self-blame for abandoning their families. Recent studies have shown increased rates of depression and anxiety symptoms among healthcare workers following the COVID-19 outbreak…
Research suggests that interventions based on social contact, which involve direct contact with individuals of the stigmatised group, are the most effective way to reduce stigma towards treatment and increase treatment-seeking intentions… Studies have shown that video and in-person interventions have similar efficacy in improving attitudes towards mental illness. Video-based interventions have benefits in cost, resource use, implementation and dissemination. Importantly, no study to date has examined the efficacy of social contact-based interventions in changing treatment-seeking attitudes among healthcare workers.
So begins a paper by Amsalem et al.
Here’s what they did:
- The authors conducted “a randomised controlled study to test the efficacy of a brief video-based intervention for increasing treatment-seeking intentions among healthcare workers, who were assessed for current levels of clinical symptoms.”
- Recruitment took place in September and October, 2020.
- Inclusion criteria: that participants speak English, be US-resident healthcare workers, and be adults.
- “Healthcare workers were randomised to (a) a brief video-based intervention at day 1, coupled with a booster video at day 14; (b) the video at day 1 only; or (c) a non-intervention control.”
- The video: “A female nurse described difficulty coping with stress, her anxieties and depression, barriers to care and how therapy helped her.” The video was just 3 minutes long, and drew from a longer interview with this nurse.
- “Treatment-seeking intentions, the primary outcome measure, were measured using three ‘openness to help-seeking’ items from the Attitudes Towards Seeking Professional Psychological Help Scale (ATSPPH-SF). The ATSPPH-SF is the most widely used assessment of treatment-seeking attitudes.”
- Statistical analyses were done.
Here’s what they found:
- “Of the 350 healthcare workers, 281 (80%) reported probable anxiety, depression and/or PTSD.”
- Demographics: most participants were female (74%); the mean age was 34.8 years; most participants were White (73%).
- Occupation: participants were mainly nurses (68%), but also physicians (15%) and emergency medical technicians (9%).
- “The brief video-based intervention yielded greater increases in treatment-seeking intentions than the control condition, particularly among participants in the repeat-video group.” See figure below.
- “Exploratory analysis revealed that in both video groups, we found greater effect among nurses than non-nurses.”
Our randomised controlled trial examined the efficacy of a brief intervention in increasing treatment-seeking intentions among healthcare workers who were assessed for self-reported anxiety, depression and PTSD. As hypothesised, the brief video-based intervention increased treatment-seeking intentions in the two video-based intervention groups, with longer-term effect noted for the video + booster group.

A few thoughts.
- This is a good study.
- To summarize: the intervention worked.
- It’s difficult not to like the approach: a low-cost intervention that can be scaled up easily. The “ask” of providers was relatively light: a few minutes to watch a video (or two).
- Like all studies, there are limitations. The sample itself was not necessarily representative of healthcare workers. The authors write: “The sample is limited to Amazon Mechanical Turk participants, who might differ demographically or clinically from the healthcare population, and it includes mostly nurses (68%) and women (74%), thus limiting generalisability.”
- As we consider our post-pandemic world, this study is very relevant and practical. How can we reach those who are struggling in the healthcare world? The authors have an intervention that can be rapidly deployed and works.
The full BJP paper can be found here:
Selection 2: “Sustained Care Smoking Cessation Intervention for Individuals Hospitalized for Psychiatric Disorders: The Helping HAND 3 Randomized Clinical Trial”
Richard A. Brown, Haruka Minami, Jacki Hecht, et al.
JAMA Psychiatry, 5 May 2021
![]()
Individuals with serious mental illness (SMI) smoke cigarettes at disproportionately higher rates, are more likely to smoke heavily, and have lower cessation rates than the general population. Adults with SMI who smoke cigarettes consume almost half (44.3%) of all cigarettes smoked in the US and have lifespans 25 to 32 years shorter than the general population. Cigarette smoking has been identified as an important modifiable risk factor for excess mortality in people with SMI.
In 2017, 3.3% of US adults, or almost 11 million adults, received inpatient psychiatric treatment in the past year. Traditionally, psychiatrists and mental health professionals have been reluctant to address cigarette smoking in their patients because of beliefs that patients are not interested in quitting smoking or concerns about the negative effects of quitting smoking on psychiatric state or recovery. However, there is growing evidence that smoking cessation may serve to improve psychiatric symptoms over the long term. Furthermore, adults with SMI who smoke cigarettes want to quit smoking and will accept smoking cessation treatment with assistance and encouragement. Psychiatric hospitalization itself has been found to increase self-efficacy and motivation to quit smoking.
While patients may be offered nicotine replacement therapy (NRT) and other medications to ease withdrawal during hospitalization, they are rarely offered quit-smoking referrals or provided with NRT on discharge, and most resume smoking after leaving the hospital…
So begins a paper by Brown et al.
Here’s what they did:
- The authors “examined the effectiveness of a multicomponent, sustained care (SusC) smoking cessation intervention in smokers with SMI receiving inpatient psychiatric care.”
- Recruitment took place between July 2015 and January 2019 at an Austin, Texas, hospital.
- Exclusion criteria included a current diagnosis of dementia and a diagnosis of a non-nicotine substance use disorder requiring detoxification.
- The intervention: “The SusC intervention included 4 main components designed to facilitate patient engagement with postdischarge smoking cessation resources: (1) inpatient motivational counseling; (2) free transdermal nicotine patches on discharge; (3) an offer of free postdischarge telephone quitline, text-based, and/or web-based smoking cessation counseling, and (4) postdischarge automated interactive voice response calls or text messages.”
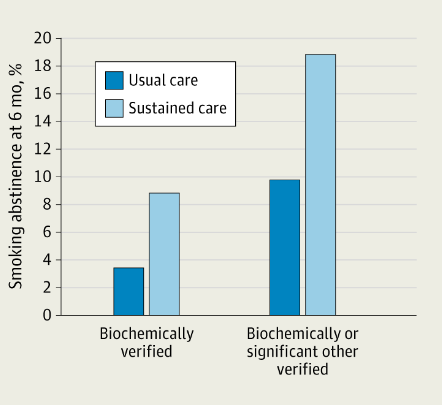
- “The primary outcome was self-reported smoking abstinence for the past 7 days (7-day PPA), verified at 6 months by saliva cotinine analysis (cutoff, ≤15 ng/mL).”
- Statistical analyses were done.
Here’s what they found:
- 353 participants were randomized; 342 were included in analyses.
- Demographics: most were White (78.4%) and male (50.6%); the mean age was 35.8.
- The mean reported smoking 16.9 cigarettes per day.
- “Participants in the SusC group evidenced significantly higher 6-month follow-up point-prevalence abstinence rates than those in the UC group (8.9% vs 3.5%; adjusted odds ratio, 2.95).” The number needed to treat was 18.5.
- “Participants in the SusC group were significantly more likely to report using smoking cessation treatment over the 6 months postdischarge compared with participants in the UC group (74.6% vs 40.5%; relative risk)…”
A few thoughts:
- This is a good study.
- The authors attempt to address a major problem: the ongoing tobacco use of so many patients with severe mental illness – a reason why life expectancy is lower in this population.
- The intervention worked. Given the damage of tobacco use disorder, a number needed to treat of 18.5 looks good; with a more liberal definition of abstinence, it was even better. Wow.
- There were several limitations, including the drop-out rate.
- And we need to temper our enthusiasm: the majority of people continued to smoke despite the intervention.
The full JAMA Psychiatry paper can be found here:
https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2779598
Selection 3: “Patients in mental healthcare should be referred to as patients and not service users”
Stefan Priebe
BJPsych Bulletin, 30 April 2021

The terms with which we name similar objects and roles can change over time. One reason may be that a term is seen as devaluing or linked with connotations that one would like to change. Psychiatry has a long history of examples of this. Terms such as ‘madness’ have been replaced by more medical terms such as ‘mental disorders’ to emphasise that one is dealing with a health problem. Another example is seen in the former asylums, which tended to change their names to avoid the negative connotations associated with a previous name that had been built up in the population over time. For example, the Karl-Bonhoeffer-Nervenklinik (last of the changed names) in Berlin changed its name four times within a period of only 100 years.
Recently, there has been a shift in the National Health Service (NHS) towards calling patients in mental healthcare ‘service users’ instead of patients.
So begins a short paper by Dr. Priebe.
He forwards four arguments; we highlight three here:
Discriminating
“When I see my general practitioner (GP) in their clinic, I am a patient. When I see the same person in a different context, we have different roles. I may be a neighbour, a fellow passenger on the same bus, a father of a child that goes to school with their child, or the GP may even be a patient in my clinic. There are endless possibilities. However, the term patient is a precise description of a temporary role in a professional health service, without any negative connotation.”
He continues: “Parity of esteem – defined as ‘valuing mental health equally with physical health’ – is undermined when mental health services use terms that distinguish their patients from patients in other services and, thus, discriminate against their own patients.”
Cynical
“Service user, as a term, suggests that the people in question either ‘use’ the services actively or that the service has been of ‘use’ to them. Neither of these assumptions necessarily applies. In England alone, more than 50 000 times a year patients are treated involuntarily, i.e. against their wishes and involving specific legislation that allows such coercion. One can hardly claim that those people ‘use’ the service, just as prisoners are not ‘prison users’.”
Patronising
“A number of surveys have asked patients in mental health services which term they prefer to be used… The majority of patients prefer the term patient, and this applies across studies that have been conducted at different times and in different settings. Insisting on a term that most of the patients explicitly do not want may be seen as patronising.”
A couple of thoughts:
- Dr. Priebe’s essay is thoughtful.
- Is it persuasive? He raises good points. Some – including service userspatients – would counter that trying to find a more empowering term isn’t a bad idea, recognizing the importance of moving past a relationship that may be overly paternalistic (at least historically). Readers can decide for themselves.
The full BJPsych Bulletin paper can be found here:
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments