From the Editor
What do you say to your patient when he insists that cannabis is helping him with his mental disorder? What is the evidence?
Of course, many papers have been published on the topic. That said, Jack Wilson (of The University of Sydney) and his co-authors contribute nicely to the literature with their new systematic review and meta-analysis – arguably the most comprehensive to date – published in Lancet Psychiatry. 54 RCTs were included, involving almost 2 500 participants, including those with depression and PTSD. “Given the scarcity of evidence, the routine use of cannabinoids for the treatment of mental disorders and substance use disorders is currently rarely justified.” We discuss the paper and its implications.

What happens to your view of our field after five decades spent treating tens of thousands of patients, leading major institutions, and authoring dozens of books and papers? In a new episode of Quick Takes, Dr. Joel Paris, former chair of the Department of Psychiatry at McGill University and a self-proclaimed skeptic, discusses the past, present, and future of psychiatry. Never one to shy away from sharing his controversial views, Dr. Paris dives into his thoughts on the DSM system (he’s not a fan) and what he sees as “fads and facilities” – such as the overdiagnosis of adult ADHD, trauma, and autism. “Over time, my perspective on psychiatry has changed in the direction of greater skepticism.”
Finally, in the third selection from The Canadian Journal of Psychiatry, Drs. Kenya A. Costa-Dookhan and Andrew Lustig (both of the University of Toronto) discuss what to do when a patient doesn’t meet criteria for an involuntary admission but isn’t well. Drawing on a case involving a patient experiencing a manic episode, they offer three strategies. “When mania outruns the law, our task is to accompany our patients with clarity, compassion, and collective integrity, not toward cure, but toward the next opportunity for care.”
DG
Selection 1: “The efficacy and safety of cannabinoids for the treatment of mental disorders and substance use disorders: a systematic review and meta-analysis”
Jack Wilson, Olivia Dobson, Andrew Langcake, et al.
The Lancet Psychiatry, April 2026

Mental disorders and substance use disorders (SUDs) are among the top contributors to the global burden of disease because of their high prevalence and inaccessibility of effective treatments. Cannabis products are increasingly becoming available for medical use and gaining attention as alternative treatments for mental disorders and SUDs. Phytocannabinoids, such as delta-9-tetrahydrocannabinol (THC) and cannabidiol, are potential therapeutic agents as they have been shown to modulate the endocannabinoid system, non-endocannabinoid receptors, and neurotransmitters that play a role in mental disorders and SUDs… 27% of the estimated population aged 16 – 65 years in the USA and Canada reported ever using cannabis for medical purposes, half of which were for managing their mental health. In Australian markets, where cannabinoid medicines have been legalised more recently, over one million applications have been approved for the use of these medicines and mental disorders make up six of the top ten most common indications for which they are prescribed.
So begins a paper by Wilson et al.
Here’s what they did:
- They conducted a “a systematic review and meta-analysis of randomised controlled trials (RCTs) testing the efficacy and safety of cannabinoids as the primary treatment for mental disorders or SUDs.”
- They searched several databases, including Ovid MEDLINE, for peer-reviewed articles published between January 1, 1980, and May 13, 2025.
- Two independent reviewers screened all studies and performed data extraction. “Evidence was synthesised as odds ratios (ORs) for dichotomous measures and standardised mean differences (SMDs) for continuous measures…”
- Primary outcomes: remission of disorder or reduction in disorder symptoms.
- “Safety was assessed via synthesis of all-cause and serious adverse events, which was used to calculate the number needed to treat to harm (NNTH).”
Here’s what they found:
- 54 trials were identified for inclusion involving 2 477 participants.
- Demographics. The majority were male (69%) with a median age of 33.3 years.
- Disorders. “Our meta-analysis revealed that a combination of cannabidiol and delta-9-tetrahydrocannabinol reduced cannabis withdrawal symptoms (SMD –0.29…) and weekly grams of cannabis use (–1.00…) among those with cannabis use disorder, and a reduction in tic severity among those with tic or Tourette’s Syndrome (–0.68…) compared with placebo. Any cannabinoid type led to an increase in sleep time as recorded by an electronic device (0.54…) and sleep diary (0.55…) among those with insomnia. There was a reduction in autistic traits (–0·36…) among those with autism spectrum disorder.”
- Other disorders. “There were no significant effects on outcomes associated with anxiety, anorexia nervosa, psychotic disorders, post-traumatic stress disorder, and opioid use disorder.”
- Lack of data. “There were insufficient data to meta-analyse studies of ADHD, bipolar disorder, obsessive-compulsive disorder, and tobacco use disorder. There was an absence of RCT evidence for the treatment of depression.” (!!)
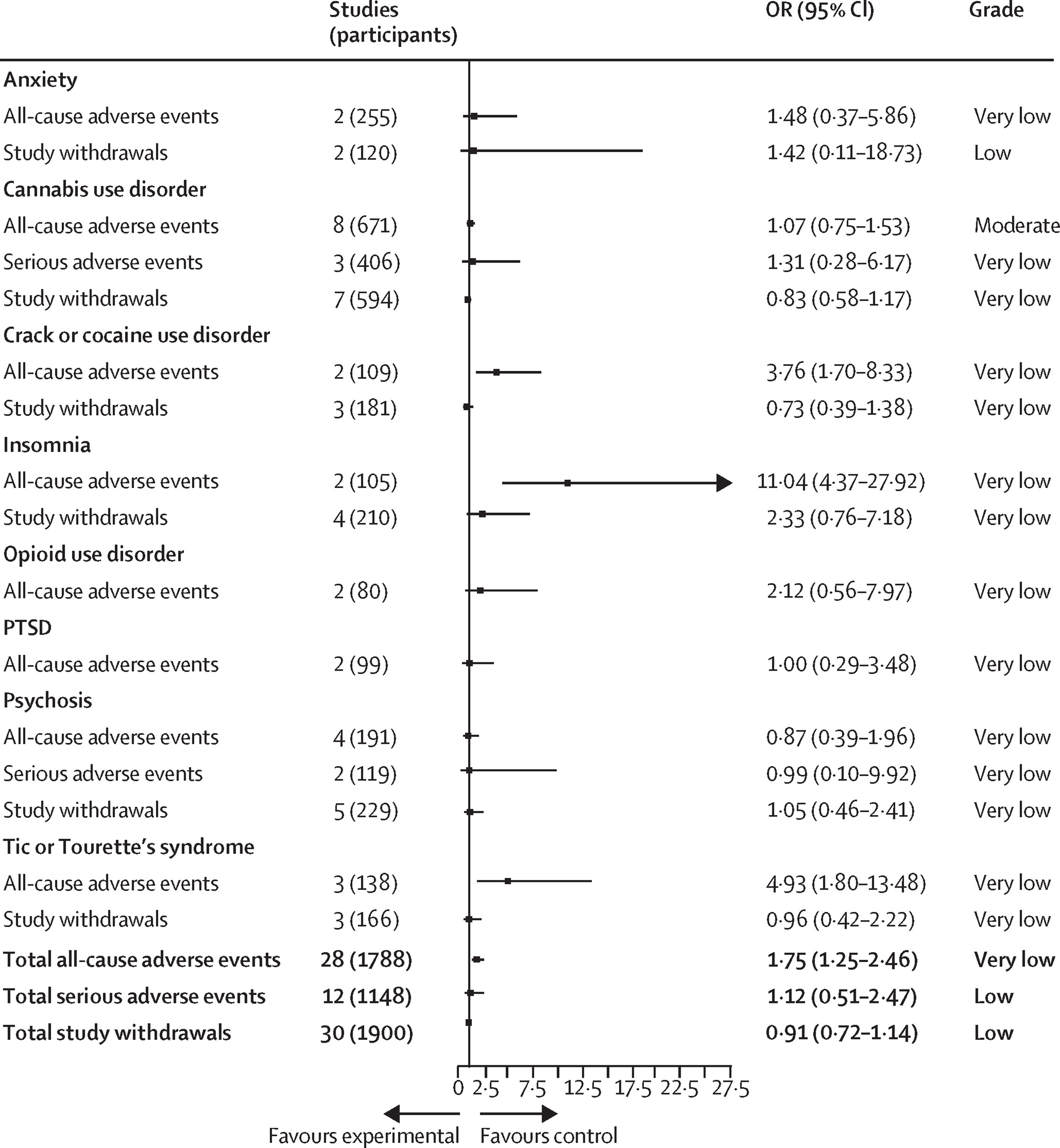
- Adverse events. “Meta-analysis revealed higher odds of all-cause adverse events (OR 1.75…) among those using cannabis versus control group (NNTH=7) but no higher odds of serious adverse events or study withdrawal.” See figure below.
- Quality. “44% of these trials had a high risk of bias, and the certainty of evidence for most outcomes was low.”
A few thoughts:
1. This is an important and relevant paper, published in a major journal.
2. The main findings: “Meta-analysis found no benefit of cannabinoids for opioid use disorder, tobacco use disorder, cocaine use disorder, bipolar disorder, anxiety, ADHD, psychotic disorders, PTSD, OCD, or anorexia nervosa. Cannabinoids were associated with a reduction in withdrawal symptoms and cannabis use among those with a cannabis use disorder and in a reduction in autistic traits among those with autism spectrum disorder. However, according to GRADE, there was very low certainty in the evidence for a reduction in autistic traits, and both studies contributing data to this outcome exhibited a high risk of bias. There was also a reduction in insomnia symptoms and some evidence of an improvement in sleep time. We identified a reduction in tic severity among those receiving cannabinoids, but only for those administered cannabidiol and THC in combination.”
3. Despite the enthusiasm of some patients (stoked by a private industry), evidence is limited. A 2022 paper found that many in North America use medical cannabis for anxiety, depression, PTSD, and sleep disorders; this Wilson et al. paper suggests limited evidence for its efficacy for those conditions.
4. “Overall, there is a crucial need for more high-quality research.” (!)
5. Like all studies, there are limitations. The authors note several, including “focused on outcomes at the longest follow-up, whereas some studies might have observed varying effects at multiple time points.”
6. Circling back to the beginning of this week’s Reading, what do you say to a patient who insists on the usefulness of cannabis for his mental disorder? Well, the evidence so far doesn’t much favour his position.
The full Lancet Psychiatry paper can be found here:
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(26)00015-5/fulltext
Selection 2: “A skeptic’s view of psychiatry”
Joel Paris
Quick Takes, 8 April 2026

In this episode of Quick Takes, I speak with Dr. Paris.
Here, I highlight several comments:
On his training and skepticism
“I was trained in the late 60s and early 70s. And at that time, there were really two psychiatries. Because I trained mostly in places where psychotherapy was the basis of thinking about patients, I was psychodynamically oriented for many years. I became very skeptical about it. I even wrote books saying why it’s wrong and misguided.
“On the other hand, I’m also skeptical about a reductionistic biological psychiatry. We don’t know enough about the brain. Neuroscience doesn’t have the answers. It’s a very immature science, and we can’t explain much about psychopathology yet. So the two psychiatries are still separate after all these years and I’m skeptical of both. But I believe in the biopsychosocial model which attempts to integrate them.”
On DSM-5
“People have come to believe that this actually describes psychopathology in an accurate scientific way and it doesn’t. It just lists of symptoms. I’m a critic of the DSM system and the ICD system isn’t really all that different. The diagnoses we use are not real things. They’re just ways of talking or categorizing things for our convenience.
“I’m also critical of the expansion of diagnoses. There was a time when everybody was bipolar if they were just moody. Now the latest thing is adult ADHD, which is being terribly overdiagnosed.”
On PTSD and trauma
“PTSD is obviously a thing, but most people who are exposed to serious trauma don’t develop PTSD. It’s an average 5 to 10% of those exposed will develop these symptoms. And that means the vast majority don’t get them. Even combat in war is a below 20%; most soldiers don’t develop PTSD. H.L. Mencken, an American journalist, said: ‘for every complex problem, there’s a simple solution that’s wrong.’”
On evidence
“I think the biggest change in psychiatry is that it is much more evidence based even than in the past. It used to be people would just talk about their clinical experience or a series of cases they’d seen and try to draw general conclusions from that. We’re more humble and we should be.”
The above answers have been edited for length.
The podcast can be found here, and is just over 23 minutes long:
Selection 3: “When Mania Outruns the Law: Managing Risk in the Liminal Zone”
Kenya A. Costa-Dookhan and Andrew Lustig
The Canadian Journal of Psychiatry, 23 March 2026 Online First

Mr A is a 34-year-old man with bipolar I disorder, admitted for mania. Over several days, he has slept only 2 h per night, has pressured speech, and has been buying large quantities of Bitcoin. When his family expresses concern, he insists that he is ‘better than ever’ and refuses all medication, despite previously being stable on his medication. He is not threatening harm to himself or others, and he is eating. Mr A’s family and friends remain torn about what the next steps are to support him.
He is voluntarily admitted to an inpatient psychiatric unit. However, when he learns that he cannot smoke cigarettes on the unit, he demands immediate discharge. The team believes he is on the verge of a significant reputational, financial, and interpersonal catastrophe, yet the criteria for involuntary admission are not met. He signs out against medical advice and is arrested within a week for public mischief. His family and friends are left devastated and deeply worried about his future.
The vignette describes a common inpatient scenario in which patients experiencing mania are acutely unwell but do not meet legal criteria for involuntary admission.
So begins a paper by Drs. Costa-Dookhan and Lustig.
They coin the phrase liminal zone to refer to the space “where clinicians must balance autonomy, safety, and therapeutic obligation despite foreseeable harm and limited legal authority.” They add: “These situations are often equally distressing for families and friends, who may recognize the impending consequences of mania yet lack any formal authority to intervene.”
“The liminal zone arises when patients do not meet criteria for a certificate of involuntary admission despite ongoing concern.”
They note the complexity. “With liminal-zone patients, teams may struggle with whether to certify, sometimes revisiting this decision repeatedly. Over-reach brings its own harm, as involuntary admission, when not clearly warranted, can worsen trust and outcomes.”
They suggest three strategies.
Strategy 1: Values-Based Containment
“When traditional legal leverage is unavailable, clinicians must leverage the patient’s own motivations. This strategy, which we call values-based containment, can buy crucial time for insight to return and medication to take effect. This can be done by framing hospitalization in the patient’s own language, for example, by focusing on how leaving prematurely may jeopardize valued domains such as work, relationships, or reputation. By translating risk into ego-syntonic terms, clinicians can sometimes re-establish temporary alignment.”
They also note the importance of recruiting allies. “Family and close supporters can often articulate the patient’s values and should be engaged early to support containment.”
Strategy 2: Preparing a Soft Landing
“If discharge is inevitable for the liminal-zone patient, the goal shifts to maximizing continuity of care and creating a therapeutic exit. This includes timely outpatient follow-up, clear rapid readmission pathways, communication with community providers, careful documentation of why involuntary admission criteria were not met despite clinical concern, the foreseeable risks identified, and the mitigation strategies attempted, which is central to good clinical care.”
Strategy 3: Containing the Team’s Distress
“Liminal situations create moral tension for staff and can fracture teams in subtle ways. Because insight and cooperation fluctuate, different team members often see different ‘versions’ of the patient. For example, the psychiatrist may encounter an irritable, grandiose patient demanding discharge at morning rounds, while the recreational therapist an hour later reports cooperative engagement in group activities. When patients appear to defy the expertise, authority, and care of the clinical team, these dynamics may elicit anger, resentment, or countertransference reactions among staff. Explicitly acknowledging and discussing these responses during team huddles or treatment planning meetings is essential to maintaining cohesion, supporting reflective practice, and preventing emotionally driven clinical decision-making.”
A few thoughts:
1. This is a practical and thoughtful paper.
2. The term liminal zone is excellent.
3. The comment about involving family is important. Some of the toughest conversations of my career have involved discussions with family members who can, understandably, see the illness of their loved one but struggle to appreciate the confines of the law.
The full Canadian Journal of Psychiatry paper can be found here:
https://journals.sagepub.com/doi/10.1177/07067437261433736
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
April 12, 2026 at 1:12 pm
Hey DG I just came up on this blog again after a while. Love everything about it and a great reminder of my days on the floor. Hope you are well.
Congrats on the new gig. Sinai is lucky to have you.
April 18, 2026 at 3:10 am
I am very impressed with this article.