From the Editor
It could be lifesaving for those with diabetes. And many others are taking GLP-1 receptor agonists, ranging from people with medical conditions such as obesity to those who have cosmetic interests. GLP-1 receptor agonists are having a moment. Could they also be helpful for patients with substance problems? Some small studies suggest yes.
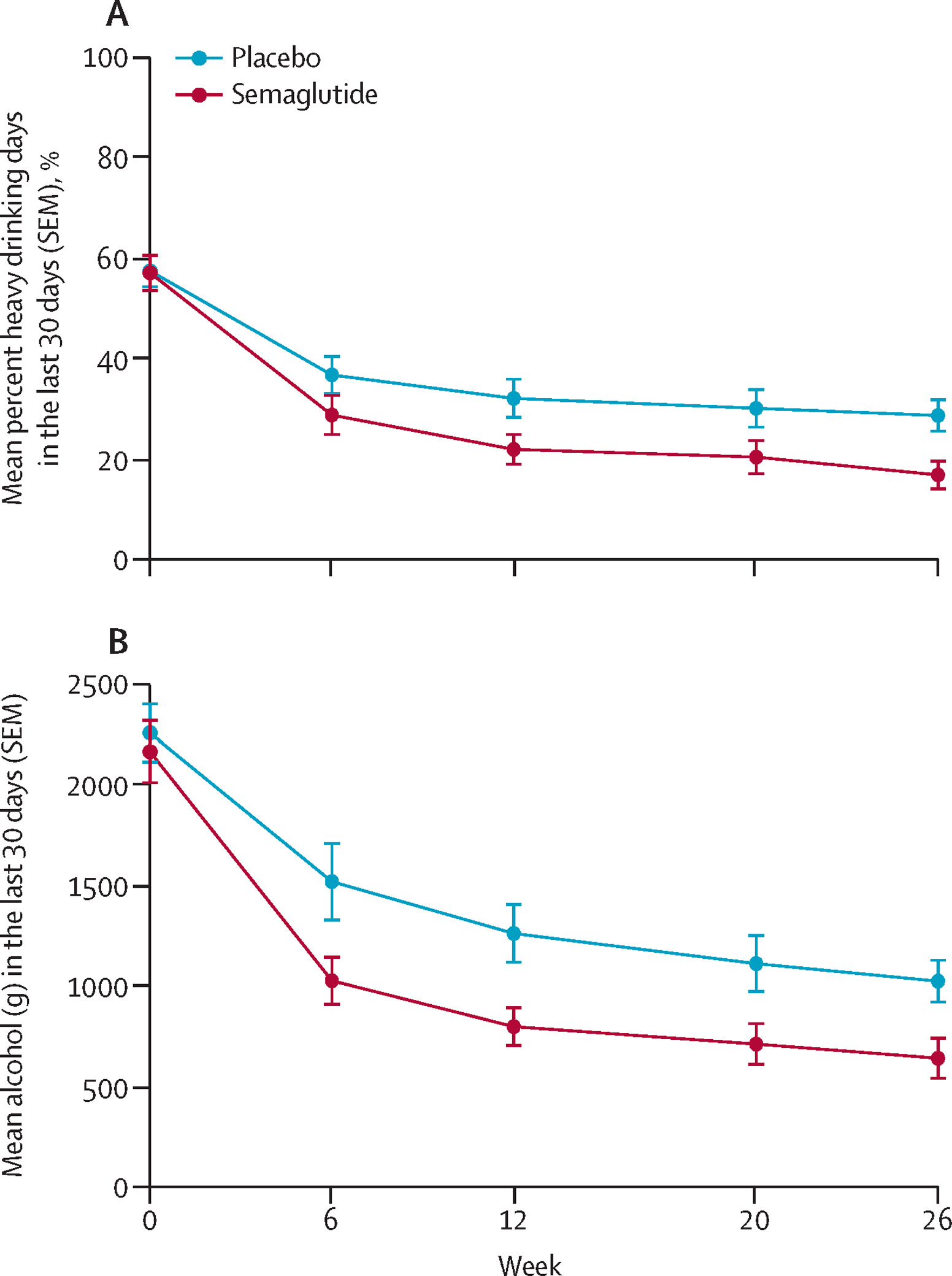
In a major new Lancet study, Dr. Mette Kruse Klausen (of Copenhagen University) and her co-authors attempt to answer that question. They report on a RCT involving patients with both obesity and alcohol use disorder. 108 Danish participants were randomized to the GLP-1 receptor agonist semaglutide or placebo. At six months, adults taking semaglutide reported five heavy drinking days in the previous months (down 41%) compared to nine days in the placebo group. “To our knowledge, this RCT is the first to show that once-weekly semaglutide reduces heavy drinking days and WHO drinking-risk levels in treatment-seeking patients with alcohol use disorder and comorbid obesity.” We consider the paper, the accompanying editorial, and its implications.

In this week’s other selection, a Viewpoint paper from JAMA Pediatrics, Drs. Lester Liao (of McGill University) and Eric Fombonne (of the Oregon Health & Science University) write on autism and overdiagnosis. “Diagnostic practices geared to accessing resources, incorrect diagnostic practices, increased attention, changes to diagnostic criteria and thresholds, and fundamental cultural shifts have contributed.”
DG
Selection 1: “Once-weekly semaglutide versus placebo in patients with alcohol use disorder and comorbid obesity: a randomised, double-blind, placebo-controlled trial”
Mette Kruse Klausen, Signe Keller Justesen, Julie Niemann Pedersen, et al.
The Lancet, 2 May 2026

Alcohol use disorder is a chronic, relapsing brain disorder characterised by loss of control of alcohol consumption and compulsive use. Several behavioural and psychological treatments are available, and cognitive behavioural therapy (CBT) is among the treatments with the highest empirical support. However, despite decades of research, the US Food and Drug Administration (FDA) has approved only three medications – disulfiram, acamprosate, and naltrexone – highlighting the urgent need for more effective treatments. GLP-1 receptor agonists, approved for the treatment of diabetes and obesity, have gained wide attention for their effects on brain pathways involved with appetite regulation and reward, suggesting potential use for mitigating alcohol consumption…
Several GLP-1 receptor agonists have shown significant reductions in alcohol consumption, reward-processing, and relapse-like behaviours, demonstrating robust and promising effects in preclinical models of alcohol addiction. In humans, register-based studies have reported a lower risk of alcohol-related events or alcohol use disorder diagnosis among individuals treated with a GLP-1 receptor agonist. Recently, a randomised controlled trial (RCT) that included 48 non-treatment-seeking participants with alcohol use disorder – characterised by lower alcohol use disorder severity, fewer alcohol-related consequences, and less motivation to reduce alcohol consumption – received low-dose semaglutide for 2 months. The study showed a significant reduction in alcohol consumption in a laboratory-based alcohol self-administration task, and decreases in drinks per drinking day and alcohol craving, compared with placebo. To our knowledge, only one RCT has evaluated the effects of a GLP-1 receptor agonist (once-weekly exenatide) in treatment-seeking patients with alcohol use disorder. No overall difference in the number of heavy drinking days was observed…
Here’s what they did:
- They conducted a “randomised, single-centre, double-blinded, placebo-controlled, clinical trial” at the Mental Health Center Copenhagen.
- Participants had moderate to severe alcohol use disorder and comorbid obesity.
- They were assigned (1:1) to “receive once-weekly semaglutide (2.4 mg subcutaneously) or placebo (saline subcutaneously), in addition to standard cognitive behavioural therapy.”
- The primary endpoint: “a reduction in the number of heavy drinking days assessed after 26 weeks of intervention, analysed with an ANCOVA model.”
Here’s what they found:
- 108 participants were enrolled, with 54 participants in each of the semaglutide and placebo treatment groups.
- Demographics. Participants included 53 women and 55 men. The vast majority were White (91% in the semaglutide group; 98% in the placebo group), and the mean age was early 50s. Most met criteria for severe alcohol use disorder (80% and 91%).
- Completion. 81% completed the full intervention.
- Reduction. Semaglutide was associated with a reduction in heavy drinking days (–41.1 percentage points from baseline) compared with placebo (–26.4, estimated treatment difference –13.7 percentage points).
- Secondary measures. “For the secondary alcohol consumption outcomes, semaglutide led to greater improvements than in those receiving placebo across multiple measures.” These included: mean total alcohol consumption and mean drinks per drinking day.
- Adverse events. These were transient, “generally mild to moderate gastrointestinal effects, and occurred more frequently in the semaglutide group.”
A few thoughts:
1. This is a good study in a major journal, addressing a practical question. There is much to like, including the RCT design.
2. The key finding in a sentence: “Semaglutide showed robust therapeutic effects in treatment-seeking participants with obesity and alcohol use disorder and this trial supports previous preclinical and clinical findings suggesting GLP-1 receptor agonists as a potential novel treatment target for alcohol use disorder.”
3. Wow.
4. Of course, perspective is important. The participants had alcohol use disorder, yes, and also obesity. As the authors note: “The inclusion criterion of BMI of 30 kg/m2 or higher limits the generalisability of the findings to the entire population of patients with alcohol use disorder.” It’s a major limitation, of course, and suggests that the main finding isn’t directly applicable to a person with alcohol use disorder but without obesity.
5. The paper is published with an accompanying Comment paper, “GLP-1 therapies: an emerging approach for alcohol reduction?” Christian S. Hendershot (of the University of Southern California) and Dr. Klara R. Klein (of the University of North Carolina) begin: “the authors present timely and compelling data indicating efficacy of semaglutide, GLP-1 receptor agonist and incretin therapy, for alcohol use disorder.”
They note the major findings. “Relative to placebo, semaglutide not only reduced heavy drinking days, but led to reductions in multiple secondary outcomes, including alcohol craving, drinks per drinking day, total alcohol consumption, and alcohol exposure biomarkers. Notably, semaglutide significantly increased the likelihood of achieving a 2-level reduction in WHO risk drinking level, a clinical trial endpoint recently qualified by the US Food and Drug Administration (FDA), with a number-needed-to-treat of 4.3 – suggesting potentially greater efficacy relative to existing alcohol use disorder medications.” (!)
They see practical applications:
“GLP-1 therapies could prove effective for reducing drinking levels in mild or prodromal alcohol use disorder, perhaps offering a treatment that can be delivered in primary care.”

Christian S. Hendershot
They do note unanswered questions and offer a cautionary note:
“Questions exist about so-called post-treatment rebound effects, and whether sustained GLP-1 receptor agonist treatment is required to maintain gains, as has been shown in metabolic disease. Studies with pre-planned, extensive follow-up are essential. The trial results also indicated individual variability, with some participants showing little or no drinking reduction, which highlights the need to understand predictors of response. Mechanisms for reductions in craving and consumption also remain to be clarified: although preclinical and initial human evidence implicates central mechanisms, the relative contribution of central versus peripheral effects requires investigation. Neuroimaging data from this and forthcoming semaglutide trials will be informative. Replicability and translation in real-world practice settings, including settings in which weekly visits and cognitive behavioural therapy are not possible, are yet to be determined.”
The full Editorial can be found here: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(26)00305-3/fulltext
6. The point about sustainability is a good one. We can also wonder about the strength of blinding given the rich side effect profile of semaglutide. Still, the study is strong.
The full Lancet paper can be found here:
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(26)00305-3/fulltext
Selection 2: “Autism Overdiagnosis and Its Harmful Effects”
Lester Liao and Eric Fombonne
JAMA Pediatrics, 13 April 2026 Online First

Autism diagnoses have been on the rise. An increasingly relevant factor to consider in growing prevalence is overdiagnosis. By overdiagnosis, we refer to a misdiagnosis or a diagnosis of a profile that is mild and not significantly impairing.
So begins a paper by Dr. Liao and Fombonne.
They list reasons that overdiagnosis occurs:
- “Diagnostic substitution contributes to increasing prevalence, specifically decreasing intellectual disability diagnoses and rising autism diagnoses.”
- “Clinicians may stretch diagnostic boundaries to access supports that would otherwise be unavailable without an autism diagnosis.”
- “Standardized diagnostic tools like the Autism Diagnostic Observation Schedule, Second Edition, and Autism Diagnostic Interview–Revised may be used and interpreted incorrectly.”
- “Different standards of screening or evaluation lead to disproportionate diagnosis across different regions.”
“Close to half of children who received autism diagnoses in the community did not meet autism criteria when reevaluated by an autism research team.”
They note three harmful repercussions.
Overdiagnosis leads to resource dilution
“There are only so many public sites and professionals for evaluation of autism and therapeutic intervention. Overdiagnosis diverts resources from children with the most significant challenges. Importantly, it is often those who are better resourced, whether in terms of cultural capital or functional capabilities (eg, the capacity to speak and self-advocate), who can navigate the medical system to ensure milder diagnoses receive supports. This leaves the most vulnerable –those who cannot self-advocate and exhausted families caring for their children full-time – without the support they need.”
The expansion of the term autism risks trivializing children with profound autism
“The spectrum diagnosis has benefits, but it loses precision. A child with social and behavioral quirks is quite different from one who does not speak, isolates himself, and frequently self-injures. Furthermore, many people will encounter milder autism but never encounter profound autism. The latter presentation is rarer, and these children tend to be in segregated settings, whether in specialized education or because behavioral profiles make public settings challenging. Thus, to speak of ‘autism’ today and bring to mind the former but not the latter child exacerbates resource diversion. The latter child is barely even known to exist.”
Medicalization increasingly lumps typical or transient behaviors into medical categories such as autism
“A self-fulfilling prophecy can develop. A child who is socially withdrawn is permitted to isolate, minimizing habituation to social circumstances and decreasing social opportunities, thereby reducing social practice. The same applies to behavioral rigidities or sensory aversions. There is a risk of attributing all the child’s troubles to autism, as opposed to, say, a circumstance, thereby reinforcing one’s concept of the child. This does not allow a child to develop their full capacity.”
They add: “Diagnostic practices geared to accessing resources, incorrect diagnostic practices, increased attention, changes to diagnostic criteria and thresholds, and fundamental cultural shifts have contributed. This can harmfully divert resources from children with greater needs, marginalize those with autism already at the periphery of our societies, and reshape the way children develop in ways that stunt natural resilience and growth.”
A few thoughts:
1. This is a thoughtful Viewpoint.
2. “There’s a significant difference between a child who has difficulty doing something and a child who utterly cannot. A spectrum does not negate this. Even on the taller end, there’s still a world of difference between being 7 or 6 ft tall.” Good point and well phrased.
3. How to proceed? They offer an agenda: Overdiagnosis can be mitigated by “(1) reliance on several informants or data sources, (2) supplementing the evaluation of current functioning with earlier data points that confirm a trajectory of autistic symptomatology, (3) demonstrating that functional impairment results from autism as opposed to co-occurring conditions or contextual constraints, and (4) providing a clinically informed and validated procedure to integrate all measurements.” Solid.
4. But in many healthcare systems, an autism diagnosis is the difference between access to services and no services. Is it surprising that providers then lean towards diagnosis?
The full JAMA Pediatrics paper can be found here:
https://jamanetwork.com/journals/jamapediatrics/article-abstract/2847690
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
May 14, 2026 at 2:59 am
I appreciate the information you shared.