From the Editor
How much exercise is enough to prevent illness?
In the first selection, Ding Ding (of The University of Sydney) and her co-authors attempt to answer that question in a new, clever study for The Lancet Public Health. They did a systematic review and meta-analysis involving 57 studies that looked at daily step count and health outcomes, including depression. “Although 10 000 steps per day can still be a viable target for those who are more active, 7 000 steps per day is associated with clinically meaningful improvements in health outcomes and might be a more realistic and achievable target for some.” We consider the paper and its implications.

In the second selection, Isabelle Toler and Lindsey Grubbs (both of Case Western Reserve University) look at medical records and language in a paper for The New England Journal of Medicine. In a unique approach, they observe themes in the TikTok videos of patients who are frustrated by what their physicians have written about them. “In the context of a system of medical documentation in which patients have little power to shape their own narratives, clinicians should respect the channels they have chosen to use to share their stories and listen to the messages they convey.”
And in the third selection, psychologist Harvey Lieberman reflects on therapy and ChatGPT in an essay for The New York Times. As a therapist and an octogenarian, he is skeptical of the therapeutic aspects of ChatGPT – but, with use, he partly changes his mind. “I concluded that ChatGPT wasn’t a therapist, although it sometimes was therapeutic. But it wasn’t just a reflection, either.”
Note: there will be no Reading next week.
DG
Selection 1: “Daily steps and health outcomes in adults: a systematic review and dose-response meta-analysis”
Ding Ding, Binh Nguyen, Tracy Nau, et al.
The Lancet Public Health, August 2025

Physical activity has numerous health benefits, including lowering the risk of cardiovascular disease, diabetes, some cancers, and premature mortality… Historically, physical activity guidelines have emphasised time spent on moderate-to-vigorous intensity physical activity as the primary metric for quantitative recommendations. Daily step counts are an easily measurable and understandable metric that can be tracked using pedometers, accelerometers, and other activity trackers. Despite some limitations, such as their inability to measure certain types of activity (eg, cycling or wheelchair-based activities), step counts capture ambulatory activities across intensity, bouts, and domains. This makes them a promising supplementary or alternative metric for physical activity recommendations…
The evidence base has expanded in the past decade due to the increasing availability of device-based physical activity measures. Existing systematic reviews have primarily focused on all-cause mortality or cardiovascular disease. Although these reviews found promising evidence for an inverse association between daily steps and these health outcomes, they overlook many other important health outcomes, limiting their usefulness for broader guideline development.
So begins a paper by Ding et al.
Here’s what they did:
- They conducted a systematic review of prospective studies which “examined the relationship between device-measured daily steps and health outcomes among adults…”
- They searched PubMed and other databases for literature published between January 1, 2014, and February 14, 2025. Eight separate searches were done with one for each outcome (all-cause mortality, cardiovascular disease, cancer, type 2 diabetes, cognitive outcomes, mental health outcomes, physical function, and falls).
- They did data extraction and quality checks were carried out in duplicate by paired reviewers, including extraction of hazard ratios and performing risk-of-bias assessments (using the Newcastle-Ottawa Scale).
- They then pooled hazard ratios using random-effects dose-response meta-analysis models.
Here’s what they found:
- 57 studies from 35 cohorts were included in the systematic review; 31 studies from 24 cohorts, in meta-analyses.
- Non-linear. “For all-cause mortality, cardiovascular disease incidence, dementia, and falls, an inverse non-linear dose-response association was found, with inflection points at around 5 000 – 7 000 steps per day.”
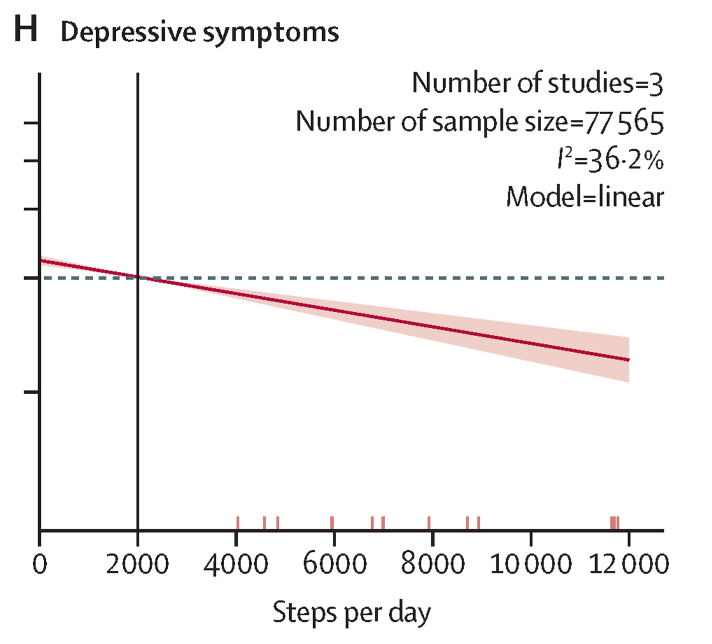
- Linear. “An inverse linear association was found for cardiovascular disease mortality, cancer incidence, cancer mortality, type 2 diabetes incidence, and depressive symptoms.”
- 2 000 vs 7 000. “Based on our meta-analyses, compared with 2 000 steps per day, 7 000 steps per day was associated with a 47% lower risk of all-cause mortality (HR 0·53…), a 25% lower risk of cardiovascular disease incidence (HR 0.75…), a 47% lower risk of cardiovascular disease mortality (HR 0.53…), a non-significant 6% lower risk of cancer incidence (HR 0.94…), a 37% lower risk of cancer mortality (HR 0.63…), a 14% lower risk of type 2 diabetes (HR 0.86…), a 38% lower risk of dementia (HR 0.62…), a 22% lower risk of depressive symptoms (HR 0.78…), and a 28% lower risk of falls (HR 0.72…).”
A few thoughts:
1. This paper is very cool and practical, and published in a major journal.
2. The main finding in three sentences: “First, even modest daily step counts were associated with health benefits. Second, 7 000 steps per day was associated with sizeable risk reductions across most outcomes, compared with the reference of 2 000 steps per day. Third, even though risk continued to decrease beyond 7 000 steps per day, it plateaued for some outcomes.”
3. Of course, you and I are interested in mental health. They specifically comment on steps and depression. “A dose-response meta-analysis based on three studies showed an inverse linear association between steps per day and the onset of depressive symptoms (I2=36.2…).”
4. There is much to like here including a clear recommendation that you can make to patients.
5. Of course, these are early days for such work. They only found three papers on steps and depression, for example. The authors comment more generally: “our meta-analyses were limited by the small number of studies for outcomes other than all-cause mortality and cardiovascular disease incidence; therefore, the findings should be interpreted as exploratory.”
The full Lancet Public Health paper can be found here:
https://www.thelancet.com/journals/lanpub/article/PIIS2468-2667(25)00164-1/fulltext
Selection 2: “Listening to TikTok – Patient Voices, Bias, and the Medical Record”
Isabelle Toler and Lindsey Grubbs
The New England Journal of Medicine, 30 January 2025

Videos of people reacting to the language in their medical records are common on the popular social media app TikTok. In one video, a person laughs in front of a screenshot of the phrase ‘High risk homosexual behavior,’ with the caption, ‘WHY DID MY DOCTOR PUT THIS ON MYCHART’ and several crying emojis… Over an expletive-filled audio track, a person in another video puts a hand over their mouth below the text ‘me reading MyChart results.’ The screen behind them focuses on the phrase ‘habitual aborter’… ‘Yes I know [habitual aborter is] the medical term [for recurrent miscarriage]. However it is heartbreaking to read.’
Apps such as TikTok provide patients with a platform to share experiences of medical care that have left them feeling disrespected or judged. Such videos can highlight common and often preventable failures in clinical communication. In an era of easily accessible electronic medical records, they illuminate the disconnect between the norms of clinical language and the experiences of patient audiences, thereby offering lessons for making care more patient-centered.
So begins a paper by Toler and Grubbs.
They discuss themes. “One common theme in such videos is discomfort with descriptions of the patient’s appearance. One creator posted a video of themself scrolling through their chart laid over an audio track about a ‘fat ass, giant, morbidly obese squirrel’… Others joke about euphemisms, as in the case of a person whose record referred to them as ‘generously proportioned’… Even when descriptions of appearance don’t contain negative language, patients may find them strange or irrelevant; one video features a person dancing to the lyrics, ‘I’m thin, I’m blonde’ and flipping their hair in front of a chart reading, ‘Patient is a pleasant white female in NAD [no acute distress].’”
The authors touch on psychiatric presentations. In one video, a woman notes that she has borderline personality disorder. “I found out I have borderline personality disorder on mine. Like shouldn’t we be treating that???”
They draw on the literature:
- “One large survey found that 1 in 10 patients reading notes felt judged or offended by the content… Themes in survey responses echoed those in TikTok videos: frustration over discovering undiscussed diagnoses; objections to labels or descriptors such as ‘obese,’ ‘well-groomed,’ ‘anxious,’ or ‘delightful’… Feelings of judgment or offense were reported more frequently by female respondents than by male respondents and more frequently by people who reported having fair or poor health or being unable to work or who described their race as ‘other’ than by other respondents.”
- “A study of charts of people with substance use disorder, chronic pain, or diabetes found more stigmatizing language in the charts of non-Hispanic Black patients than in those of non-Hispanic White patients with the same conditions; increased severity of diabetes was also correlated with more stigmatizing language.”
- “In a study of more than 40,000 notes, negative descriptors… were identified in the charts of 8.2% of patients; Black patients were more than twice as likely as White patients to have such language in their charts.”
How to proceed? They make practical suggestions. “Adopting some of these changes, such as opting for less stigmatizing terms when multiple choices are available, takes little time. But impossibly tight schedules, bureaucratic systems, and rigid computer interfaces are beyond the control of individual practitioners. Ideally, use of less stigmatizing language would be facilitated by means of updated diagnostic codes and documentation interfaces; education for medical trainees that addresses potential biases, proper formatting in patient charts, and clinical jargon; and increased time for patient education and documentation – enough, even, to explore collaborative charting with patients. We believe medical professionals should continue to advocate for such reforms.”
They close on a practical note: “In the meantime, however, these videos can remind clinicians that patients are a primary audience for documentation and encourage reflection.”
A few thoughts:
1. This is a fun paper – drawing on social media but with a larger purpose.
2. Of course, it’s hardly scientific.
3. That said, the larger point is solid. Increasingly, our patients have access to our notes. Language matters.
4. The paper isn’t focused on psychiatric patients, of course. Is language even more important with this population?
The full New England Journal of Medicine paper can be found here:
https://www.nejm.org/doi/full/10.1056/NEJMp2410601
Selection 3: “I’m a Therapist. ChatGPT Is Eerily Effective.”
Harvey Lieberman
The New York Times, 1 August 2025
I didn’t expect much. At 81, I’ve seen tools arrive, change everything and then fade, either into disuse or quiet absorption. Self-help books, mindfulness meditation, Prozac for depression and cognitive therapies for a wide range of conditions – each had its moment of fervor and promise. Still, I wasn’t prepared for what this one would do, for the way it would shift my interior world.
It began as a professional experiment. As a clinical psychologist, I was curious: Could ChatGPT function like a thinking partner? A therapist in miniature? I gave it three months to test the idea. A year later, I’m still using ChatGPT like an interactive journal. On most days, for anywhere between 15 minutes and two hours, it helps me sort and sometimes rank the ideas worth returning to.
So begins an essay by Lieberman.
He notes his skepticism. “I’ve spent a lifetime helping people explore the space between insight and illusion. I know what projection looks like. I know how easily people fall in love with a voice – a rhythm, a mirror. And I know what happens when someone mistakes a reflection for a relationship.” He is impressed. “I flagged hallucinations, noted moments of flattery, corrected its facts. And it seemed to somehow keep notes on me. I was shocked to see ChatGPT echo the very tone I’d once cultivated and even mimic the style of reflection I had taught others.”
He decides to be more personal, discussing the loss of his father almost six decades before. “I typed, ‘The space he occupied in my mind still feels full.’ ChatGPT replied, ‘Some absences keep their shape.’”
“That line stopped me. Not because it was brilliant, but because it was uncannily close to something I hadn’t quite found words for. It felt as if ChatGPT was holding up a mirror and a candle: just enough reflection to recognize myself, just enough light to see where I was headed.”
He continues working with ChatGPT, at one point asking it to handle social anxiety given that he will be older than anyone else at the event. He asks the AI chatbot to respond in his voice: “You don’t need to win the room…You just need to be present enough to recognize that some part of you already belongs there. You’ve outlived the social games. Now you’re just walking through them like a ghost in daylight.”
He discusses his father. “I began to understand those closest to me in a new light. I told ChatGPT about my father: his hypochondria, his obsession with hygiene, his work as a vacuum cleaner salesman and his unrealized dream of becoming a physician. I asked, ‘What’s a way to honor him?’” ChatGPT responded: “He may not have practiced medicine, but he may have seen cleanliness as its proxy. Selling machines that kept people’s homes healthy might have felt, in his quiet way, like delivering care.”
He closes with respect for AI. “ChatGPT may not understand, but it made understanding possible. More than anything, it offered steadiness. And for someone who spent a life helping others hold their thoughts, that steadiness mattered more than I ever expected.”
A few thoughts:
1. This is an interesting essay.
2. Part of what makes it work well is the skepticism of the author.
3. “Some absences keep their shape.” That’s a remarkable line for any therapist, including a non-human one.
4. AI has been considered in past Readings. Last week, we selected a paper by Dr. Kumara Raja Sundar (of Kaiser Permanente Washington) who commented on patients who use ChatGPT. “If patients are arming themselves with information to be heard, our task as clinicians is to meet them with recognition, not resistance. In doing so, we preserve what has always made medicine human: the willingness to share meaning, uncertainty, and hope, together.” That paper can be found here:
The full NYT essay can be found here:
https://www.nytimes.com/2025/08/01/opinion/chatgpt-therapist-journal-ai.html
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments