From the Editor
With more and more countries legalizing cannabis, we must wonder about the health implications. This week’s Reading offers three selections.
How does legalization (and increased use) affect mental health? Is there more psychosis? In the first selection, just published in CMAJ, Dr. Daniel T. Myran (of the University of Toronto) and his co-authors analyzed data from 12 million people born in Ontario, Canada, to attempt to answer those questions. They looked at diagnoses of psychosis-related disorders and years of birth, finding those born in the early 2000s were about twice as likely to have been diagnosed with a psychotic disorder by age 20. “The incidence of psychotic disorders has increased in more recent birth cohorts.” We consider the paper and its implications.

In a recent US survey, 20% of respondents reported using CBD in the last year – which is often assumed to be safer than THC. In the second selection from JAMA Internal Medicine, Jeffry Florian (of the US Food and Drug Administration) and his co-authors analyzed liver enzymes of healthy participants randomized to CBD or placebo. “In this randomized double-blinded placebo-controlled trial, 5.6% of healthy adults administered CBD 5 mg/kg/d for up to 28 days experienced liver enzyme level elevations greater than 3 times the upper limit of normal.”
Finally, in the third selection, Dr. Aaron E. Carroll (of Indiana University) writes about cannabis legalization. While arguing that there are successes with this policy change, he also worries about long-term consequences. He writes that reforms are needed, from better regulation to more education. “The real lesson here isn’t even about cannabis. It’s about our capacity to learn and adapt.”
DG
Selection 1: “Incidence of psychotic disorders by birth cohort: a population-based cohort study in Ontario, Canada”
Daniel T. Myran, Maya Gibb, Michael Pugliese, Jess G. Fiedorowicz, et al.
CMAJ, 2 February 2026

Schizophrenia is a psychiatric disorder characterized by hallucinations, delusions, negative symptoms, and cognitive impairments, typically emerging in early adulthood. Individuals living with a psychotic disorder often have comorbidities and are at a higher risk of premature death than those without the condition. Currently, about 1% of people in Canada and 0.45% of the adult global population have a diagnosis of schizophrenia. Although genetic predisposition is a key risk factor for psychotic disorders, other environmental and social factors – including air pollution, urbanization, perinatal health, early-life exposures such as adverse childhood experiences, and substance use – are thought to play a role in its development…
In Canada, the age-standardized incidence of schizophrenia has declined over the past 2 decades, from 62 per 100 000 people in 2003 to 53 per 100 000 in 2023. Importantly, this overall pattern does not account for potential birth cohort differences. Age-period-cohort (APC) studies are an established method to examine how differences in exposures by birth cohort may influence health. Such APC analyses in other regions have suggested that the incidence of schizophrenia and psychosis varies substantially across birth cohorts, potentially influenced by social and environmental factors.
So begins a paper by Myran et al.
Here’s what they did:
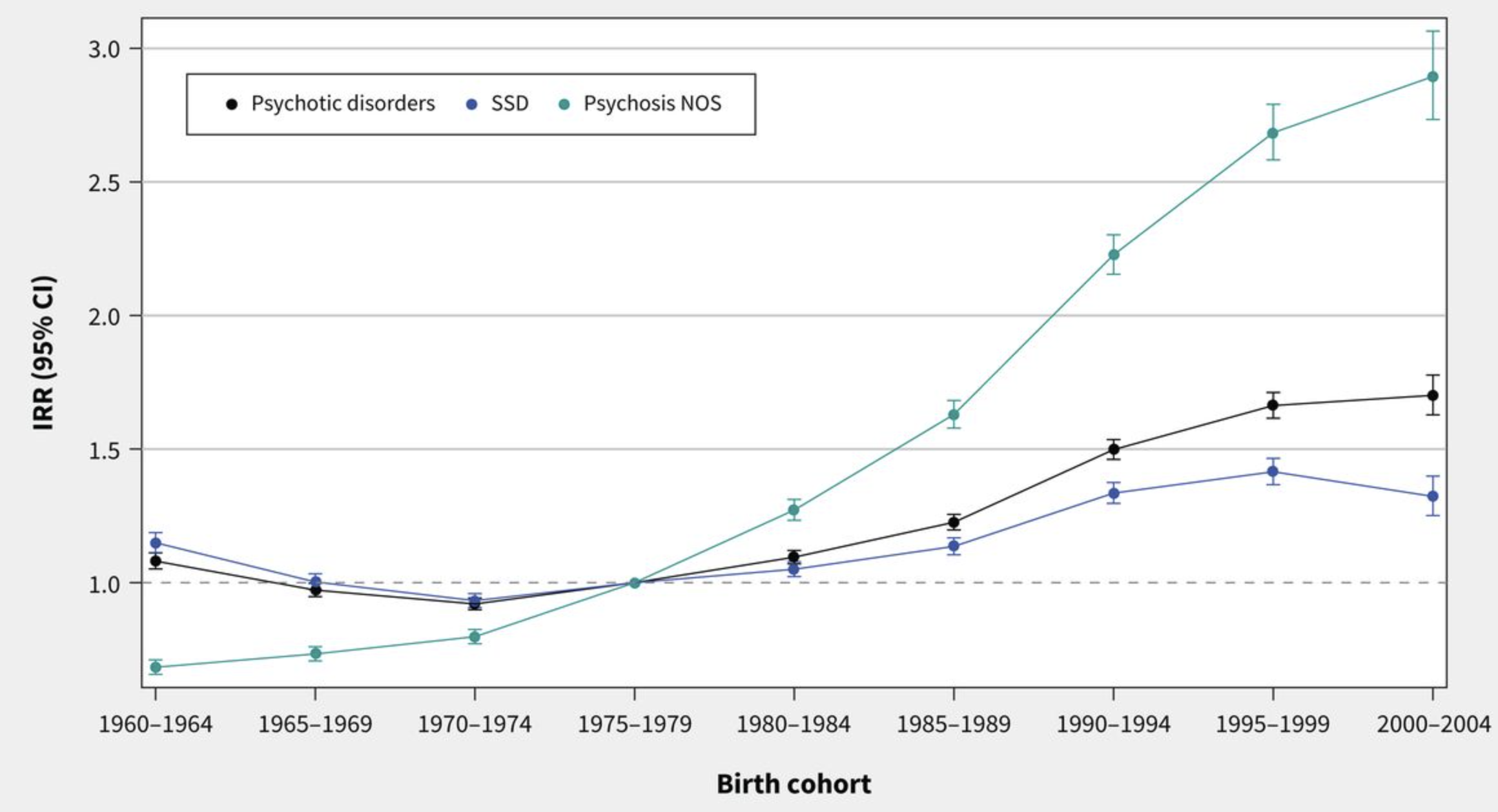
- They conducted “a retrospective, population-based cohort study using health administrative data from Ontario, Canada, between Jan. 1, 1992, and Dec. 31, 2023, to capture diagnoses of schizophrenia spectrum disorder (SSD) and psychosis not otherwise specified (NOS) – collectively, nonaffective psychotic disorders.”
- People included: those born between 1960 and 2009 who were eligible for Ontario’s Health Insurance Program and who were aged 14 to 50 years during one or more years of the study period. (97% of Ontario residents are eligible for the public insurance.)
- They then used age-period-cohort (APC) models to compare birth cohort effects, accounting for differences in age and period.
Here’s what they found:
A few thoughts:
1. This is a major paper on a timely and relevant issue, published in a respected journal.
2. The main finding in a sentence: “We found that the incidence and cumulative proportion of people diagnosed with psychotic disorders have increased in more recent birth cohorts and that the age of diagnosis has decreased in Ontario.” To add a bit more detail: it’s a major rise in those 14 to 20 years (60%). As the lead author told The New York Times: “I was expecting to see some increases in these younger folks, but I was quite surprised by the scale.”
3. This summary doesn’t quite capture the depth of the statistical analyses.
4. The authors note several reasons for the rise, including better early detection. As well, “rates of substance use – including cannabis, stimulants, hallucinogens, and synthetic drugs – have increased over time in Canada; use of these substances is associated with the development and worsening of psychotic disorders. The increase in psychosis NOS diagnoses, which are often used in the context of co-occurring substance use, may also be capturing the involvement of substance use in psychosis presentations…”
5. It’s a big finding. Is it too big? Studies drawing on North European data have found increases in the incidence of psychotic disorders in young people, but not quite so pronounced (speaking to differences in methodology, perhaps).
6. Like all studies, there are limitations. The authors note several, including the challenges of understanding different effects.
7. Cannabis has been discussed in past Readings. Recently, we considered the JAMA paper that looked at its medicinal use. “Despite the accumulation of new studies, evidence is insufficient for the use of cannabis or cannabinoids for most medical conditions.” That Reading can be found here:
The full CMAJ paper can be found here:
https://www.cmaj.ca/content/198/4
Selection 2: “Cannabidiol and Liver Enzyme Level Elevations in Healthy Adults: A Randomized Clinical Trial”
Jeffry Florian, Pablo Salcedo, Keith Burkhart, et al.
JAMA Internal Medicine, September 2025

The availability and consumer use of cannabidiol (CBD) products have increased in recent years. The cannabis plant contains bioactive compounds known as cannabinoids; delta-9 tetrahydrocannabinol (psychoactive component) and CBD (nonpsychoactive component) being the most prevalent in most varieties of cannabis…
Only one CBD human drug product (Epidiolex; Greenwich Biosciences) is approved by the US Food and Drug Administration (FDA) for the treatment of seizures associated with Lennox-Gastaut syndrome, Dravet syndrome, or tuberous sclerosis complex. At labeled doses up to 25 mg/kg/d, an increased risk of liver enzyme level elevation was observed. Liver enzyme level elevations typically occurred after 2 weeks and were dose dependent. Limited liver safety data available for lower CBD doses are inconsistent regarding the occurrence and severity of liver enzyme level elevations at 200 to 400 mg a day. Consumer self-reporting on CBD use indicates upwards of 200 mg daily, so additional safety information at these doses is needed. Further, multiple animal studies have reported CBD effects on the endocrine system, but limited human data exist.
So begins a paper by Florian et al.
Here’s what they did:
- They conducted “a randomized double-blinded placebo-controlled trial in healthy participants at a clinical pharmacology unit… evaluating the effects of daily CBD use on liver enzyme level elevations and endocrine measures at a dose within the reported range of consumers use with unregulated CBD products…”
- Inclusion criteria: age 18 to 55 years, normal medical history findings, and clinical laboratory results.
- Participants were randomized to CBD, 5 mg/kg/d or placebo for 28 days with weekly laboratory assessments.
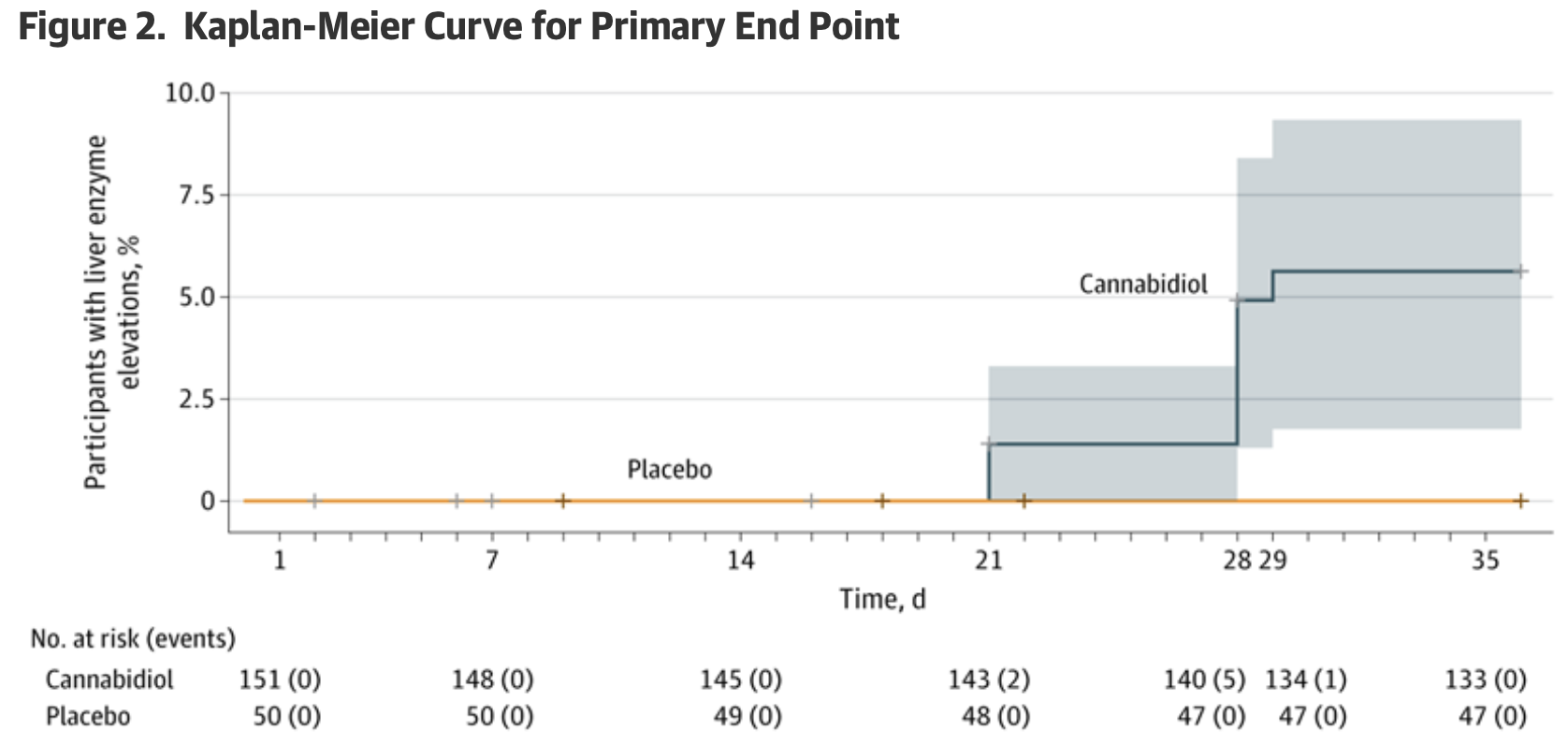
- Primary end point: “the percentage of participants with an alanine aminotransferase or aspartate aminotransferase level elevation greater than 3 times the upper limit of normal during the study.”
Here’s what they found:
- 408 healthy volunteers were screened with 201 participants were enrolled and randomized into two groups: 151 participants taking CBD solution and 50 taking placebo.
- Demographics. Participants had a mean age of 36 years; 56% were men; 49% were White.
- Liver enzymes. Among participants receiving CBD, 5.6% experienced ALT elevations exceeding 3 times the ULN, as determined by Kaplan-Meier analysis after 4 weeks of CBD dosing. No participants in the placebo arm exhibited ALT elevations meeting this threshold.
- Elevation. “Eight individuals in the CBD group who experienced ALT elevations greater than 3 times the ULN demonstrated a range of severity with 5 individuals (3.3%) experiencing peak ALT levels greater than 5 times the ULN and 2 individuals (1.3%) with ALT levels greater than 10 times the ULN, with the highest greater than 18 times the ULN…”
A few thoughts:
1. This is a good study addressing a relevant clinical problem and published in a major journal.
2. The main finding: “in this randomized double-blind clinical trial of healthy adults administered CBD, 5 mg/kg/d for 28 days, 8 (5.6%) experienced liver enzyme level elevations and 7 (4.9%) met protocol defined criteria for potential drug-induced liver injury.”
3. Is CBD use as innocuous as some – including private industry – would argue? The authors wonder. They offer practical advice: “Given the growing popularity of unregulated CBD-containing products in the market and the ability of CBD to cause liver enzyme level elevations, inclusion of CBD use as part of routine medical screening could be considered, particularly in patients with existing liver conditions or those taking medications metabolized by the liver. For patients presenting with elevated liver enzymes, CBD use could be considered in the differential diagnosis.”
4. Like all studies, there are limitations. The authors note several, including “CBD dosing of this study was within the range of reported consumer use, but on the higher end and administered twice daily.”
The full JAMA Internal Medicine paper can be found here:
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2836267
Selection 3: “Trump’s New Marijuana Policy Offers an Opportunity”
Aaron E. Carroll
The New York Times, 19 December 2025

President Trump ordered marijuana to be rescheduled under federal law on Thursday, shifting it out of the most restrictive drug category. The move would make it easier to conduct medical research on the drug, though it would stop short of federal legalization. It has reignited familiar arguments about whether cannabis is harmless or dangerous, medicine or vice, success or failure.
That debate misses the point. Instead of choosing sides, we should acknowledge that policy moved faster than the evidence on public health effects. The challenge is whether we are willing to adjust course when we encounter unintended consequences.
So begins an essay by Dr. Carroll.
“Broadly, state-level legalization of recreational marijuana, now in 24 states and D.C., did what it was expected to do. It made marijuana easier to obtain and more socially acceptable. Arrests for possession in states that legalized the drug for recreational use dropped sharply, and many fewer people are going to jail or prison for marijuana use. These outcomes should be celebrated.”
He sounds a note of caution. “But all policy decisions have trade-offs, and cannabis legalization is no exception. Recent studies show that while overall rates of severe mental illness have not surged, a growing share of new psychosis diagnoses involves people with heavy cannabis use. Other research suggests that impaired driving risk might have increased in some places, even as measurement of road safety effects and enforcement lag reality. Emergency departments are seeing more cannabis-related visits, often tied to heavy use and dependence. It’s estimated that nearly a third of adult users have reported symptoms consistent with cannabis use disorder, meaning they continue to use despite significant negative effects on their lives.”
He adds: “These harms are not evenly distributed. They cluster among heavy users, younger people and those who are already vulnerable.”
“Policy decisions often have to be made in the absence of complete evidence on their potential public health effects, especially when existing laws are clearly doing harm. Legalization reduced arrests and incarceration, but it also created a commercial market faster than we built the systems needed to monitor health effects, educate consumers or manage risk… The solution is not to call for a return to the old system but to acknowledge the need to make new policies that can address the unintended effects of legalization.”
How then to proceed? He makes several suggestions.
- Better regulation. “Today’s cannabis products are far stronger than those studied a generation ago. High-potency products should face higher taxes, stricter labeling and tighter marketing limits, much as higher-proof alcohol does.”
- Improved public education. “We must avoid scare tactics and wellness slogans. Today’s cannabis industry markets high-potency products aggressively, sometimes overstating benefits or downplaying risks. Good science communication would include honest messages that risks rise with potency, early use, frequency of use and certain mental health histories.”
- Research on impaired driving. “Blood THC thresholds do not reliably measure impairment. Officer training, including on how to observe signs of intoxication based on drivers’ behavior, and public campaigns focused on the risks of cannabis use combined with alcohol would help reduce harm.”
- Spending on care. “If cannabis is going to generate tax revenue, it should help pay for the consequences it creates. Emergency departments, early psychosis programs and treatment for cannabis use disorder should not be afterthoughts.”
- Collecting better data. “Legalization raced ahead of the surveillance of its public health consequences. States should be required to track cannabis-related emergency visits, poisonings and mental health crises. We cannot manage what we don’t measure.”
A few thoughts:
1. This is a thoughtful essay which offers constructive suggestions.
2. To borrow a line from H. R. Handelman: “Once the toothpaste is out of the tube, it is awfully hard to get it back in.” It’s unlikely that jurisdictions will go back to outlawing cannabis. Instead, he forwards a reasonable agenda.
3. Cigarettes are legal – yet are carefully regulated. Why is cannabis so different?
The full NYT essay can be found here:
https://www.nytimes.com/2025/12/19/opinion/trump-marijuana-policy.html
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments