From the Editor
It’s the most effective treatment for those with treatment-resistant depression. Older studies, including one from Quebec, suggest that it’s much less used than in the past. Is ECT going the way of the dodo bird?
In a new Canadian Journal of Psychiatry study, Dr. Tyler S. Kaster (of the University of Toronto) and his co-authors attempt to answer that question. They drew on 17 years of data, tapping several administrative databases from Ontario, covering more than 450 000 treatments. They offer some good news. “We found that while ECT use generally increased over time, there were notable differences between biological sexes, age groups, and geographic regions.” We consider the paper and its implications.

In the second selection, a research letter published in JAMA Pediatrics, Scott I. Donaldson (of Rutgers University) and his co-authors connect social media content with the desire to drink among young people. Drawing on survey data, they analyzed the impact of lifestyle influencers. “This experimental evidence adds to a growing body of research showing that exposure to alcohol-promoting content, particularly on social media, is associated with alcohol-promoting attitudes and behaviors in young adults.”
Finally, in the third selection, Pranav Jayaraman (of Texas Tech University) writes about diagnoses and patients in Academic Psychiatry. The medical student discusses the temptation to reduce experiences to simple diagnoses. “As I seek to serve patients through psychiatry, a field often facing provider capacity and time constraints, the desire to pinpoint a single cause and address it with a straightforward solution is understandable but can also be limiting.”
DG
Selection 1: “Electroconvulsive Therapy Variability Across Ontario 2007–2023: A Population Level Study”
Tyler S. Kaster, Michael A. Campitelli, Amreen Babujee, et al.
The Canadian Journal of Psychiatry, January 2026

Electroconvulsive therapy (ECT) is the most effective treatment for severe psychiatric disorders. It is particularly well-established for the treatment of severe depression with response and remission rates in the range of 60%. ECT also has evidence for reducing the risk of hospitalization, suicide and all-cause death. It can also alleviate psychotic symptoms in schizophrenia even among those resistant to clozapine…
Despite its efficacy, ECT is often underused and evidence suggests its use may be declining. Some of this decline may be related to its portrayals in the media and resulting stigma or discrimination around the procedure. Given the importance of ECT for individuals with severe psychiatric illness, there is a need to understand the population level use of ECT to ensure proper access to this life-saving treatment…While several jurisdictions have reported on population level delivery of ECT, this has not yet been reported in the province of Ontario. Furthermore, to our knowledge, only one of these studies included a period encompassing the COVID-19 pandemic… However, this study did not assess the impact of the pandemic on ECT use at the population level or within subgroups, which is particularly important given the fundamentally altered access to ECT that may have occurred.
Here’s what they did:
- They used population-level data from Ontario to examine all ECT procedures administered from 2007 to 2023; they drew on different administrative databases, including OHIP (public insurance) billings.
- The primary measure of variability was the rate of ECT procedures per 1 000 population.
- They included three subgroups at the time of ECT procedure: “age (18–39, 40–64, and 65+), biologic sex (male/female), and Ontario Health (OH) region of residence (West, Central, Toronto, East, North West, North East).”
- To quantify the impact of the COVID-19 pandemic, they calculated the change in ECT rate from 2019 to 2020 (acute effect) and from 2019 to 2023 (persistent effect).
Here’s what they found:
- There were 450 381 ECT procedures delivered in Ontario over the study period; 223 654 were for inpatients and 226 727 outpatients.
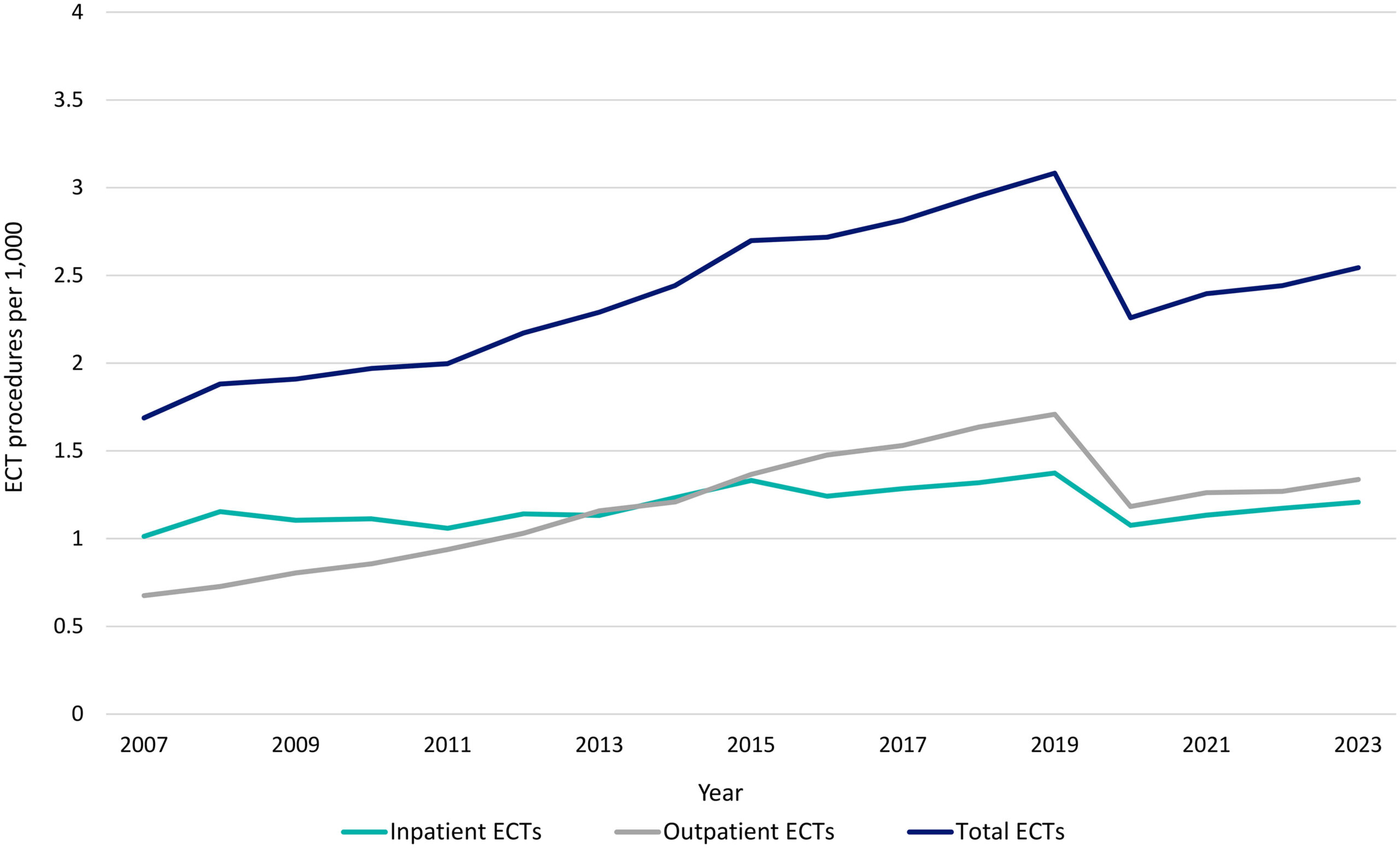
- Yearly rate. “The yearly rate of ECT increased from 1.69 per 1,000 in 2007 to a peak of 3.08 per 1,000 in 2019.” See figure below.
- Demographics. “In 2023 the greatest per capita rates of ECT use were in the 65+ age group, female sex, and North East geographic region.”
- Geography. “In 2023, the rates of ECT use in different geographic regions ranged from 1.28 (North West) to 4.19 per 1,000 (North East).” (!)
- Pandemic. “The COVID-19 pandemic resulted in an immediate 26.73%, followed by a 17.47% persistent drop in the rate of ECT with notable regional heterogeneity.”
A few thoughts:
1. This is a good study, offering interesting, relevant data, and published in a solid journal.
2. The main findings in a couple of sentences: “We found that while ECT use generally increased over time, there were notable differences between biological sexes, age groups, and geographic regions… We found that the COVID-19 pandemic has had persistent impacts on ECT delivery several years into the pandemic.”
3. Good news. ECT isn’t going the way of the dodo bird (at least in Ontario).
4. But the geographic variability is striking. How should we understand this? “The low rate of procedure use in some regions suggests that there may be individuals who could benefit from the treatment, but who are unable to access it.” Ouch. Even in a public system like Ontario’s, significant variation in care exists.
5. I’ll be provocative: would we accept that type of variation for, say, life-saving chemotherapy for some oncology patients?
6. Like all studies, there are limitations. The authors note several, including the lack of information on maintenance versus acute ECT, and on diagnoses.
7. ECT has been considered in past Readings. Dr. Rebecca E. Barchas, a retired psychiatrist, discusses her experiences with ECT – as a patient, not as a physician. She notes the depths of her depression and the decision to receive ECT, which she didn’t know much about despite many years of practice. “If reading these thoughts can help even one more patient who needs ECT accept it or help one more physician to consider recommending it when appropriate, I will have accomplished my goal of helping to destigmatize ECT.” That Reading can be found here:
https://davidgratzer.com/reading-of-the-week/reading-of-the-week-ect-at-82/
The full CJP paper can be found here:
https://journals.sagepub.com/doi/10.1177/07067437251371977
Selection 2: “Exposure to Alcohol-Related Social Media Content and Desire to Drink Among Young Adults”
Scott I. Donaldson, Alex M. Russell, and Jon-Patrick Allem
JAMA Pediatrics, 23 February 2026 Online First

Social media use is common among young adults and is characterized by a continuous stream of content from peers and influencers, which can feature alcohol in aspirational or humorous contexts. Although prior research has linked exposure to alcohol-promoting content on social media with alcohol-promoting attitudes and behaviors among young adults, most of those studies were cross-sectional, unable to establish temporal precedence, and limited by unmeasured confounding variables. Establishing experimental evidence of this association is critical for guiding social media policy. We examined whether exposure to alcohol-promoting social media posts precedes increased desire to drink among young adults.
So begins a paper by Donaldson et al.
Here’s what they did:
- They recruited US individuals aged 18 to 24 years.
- Participants were “randomly assigned to a treatment or control condition designed to simulate a typical social media browsing experience and were matched to a sampling frame; matched cases were weighted.”
- “In the treatment condition, participants viewed 20 Instagram (Meta Platforms) posts from lifestyle influencers that visibly depicted alcohol consumption or alcohol-promoting imagery (eg, holding alcoholic beverages). In the control condition, participants viewed 20 matched social media posts from the same influencers but without any alcohol-related imagery.”
- Outcome: the desire to drink which was assessed “using a single-item measure adapted from prior research.”
Here’s what they found:
- The sample included 2 000 participants.
- Demographics. The mean age was 21.2 years; 47.2% were females.
- Desire to drink. “Treatment condition participants had significantly greater odds of reporting higher desire to drink than control condition participants (adjusted odds ratio [AOR], 1.73…).”
- Influencers. “Participants who perceived influencers as highly credible compared with those who did not had greater odds of reporting higher desire to drink (AOR, 5.53…).”
- Use. “Similar direct associations between prior alcohol use and desire to drink were observed among participants who reported past 30-day alcohol use (AOR, 1.40…) and past 30-day binge drinking (AOR, 1.30…).”
- Analyses. Results were consistent across sensitivity analyses.
A few thoughts:
1. This is an interesting letter.
2. The core finding: “Exposure to alcohol-promoting social media content was associated with desire to drink across varying levels of prior alcohol use, and social media influencers may contribute to normalization of alcohol consumption among young people.”
3. There are clear limitations with this research letter. Start here: participants simply completed a one-item survey. And “desire to drink” is different from drinking. “It remains unclear whether exposure to alcohol-promoting content leads to increased alcohol consumption in this population.”
4. Still, social media casts a long shadow. Youth spend more and more time online – what are they being exposed to? Alcohol regulations in many countries cover traditional advertising. What about the work of influencers?
The full JAMA Pediatrics letter can be found here:
https://jamanetwork.com/journals/jamapediatrics/article-abstract/2845350
Selection 3: “There Are Neither Chekhov’s Guns nor Silver Bullets in Psychiatry”
Pranav Jayaraman
Academic Psychiatry, 7 February 2026 Online First

‘Ahh, I knew there must have been trauma in her youth,’ I told my supervising resident with unwarranted confidence during our debrief of a recent patient, ‘Becca.’ Only a few months into the third year of medical school, I recognized an overly reductive approach had crept into my interviews. I found myself not just asking leading questions after hearing a key ‘buzzword’ or event early on but, sometimes, as with Becca, slipping into conducting entirely ‘leading’ interviews. In this case, on the basis of factors like gender and her comments describing her father as ‘the worst ever’ that I thought were consistent with ‘splitting behavior,’ I became married to the diagnosis of borderline personality disorder. This narrow focus and my subsequent screening for trauma to reinforce my initial premature conclusion led our team interview and formulation to quickly center around the trauma, collapsing multiple possibilities into one convenient cause.
So begins a paper by Jayaraman.
She touches on Russian literature. “This pattern of thinking reminded me of the writing principle of ‘Chekhov’s gun’ from my sketch-comedy days. Russian playwright Anton Chekhov is famously credited with stating, ‘If you say in the first chapter that there is a rifle hanging on the wall, in the second or third chapter it absolutely must go off’. As a trainee, I have noticed how easy it is to fall into treating our patients’ lives like screenplays, manifesting each recognized risk factor into a clinical imperative and demanding that their complex, layered lives fit a singular, linear narrative.”
She notes the problems of “pigeonholing patients into definitive diagnoses” as she is robbed of the “chance to explore competing diagnoses or coexisting conditions.” She adds: “While borderline personality disorder could explain Becca’s mood shifts and disruptions in work performance, so could her recent lack of sleep, a competing diagnosis, or another combination of factors. More importantly, when I anchor on one part of a patient’s history and let that dictate the remainder of the interview, I am no longer listening but just confirming. How can I expect to connect with my patient if I am not truly listening? Recognizing what our patients have endured can provide timely validation, but when I prioritize causation over connection, ‘Chekhov-ing,’ I risk entirely missing the person in front of me.”
“This focus on the ever-elusive ‘underlying cause’ and ‘definitive’ diagnosis is not just limited to trainees. Attendings and board questions alike reward the recall of the typical constellation of findings and epidemiological associations. Resulting expectations can implicitly or explicitly train us to piece together risk factors and clinical clues into a ‘coherent’ narrative. Intake screenings for risk factors such as firearm ownership… are crucial for ensuring immediate patient safety and shaping our understanding of the patient’s context. However, risk factors often remain just that: risk factors.”
She returns to Becca and describes a later encounter. “She divulged she had trouble making long-term friends as a youth because her mother’s military service required constant relocation. She then used gaming online as an adult, often late at night, to maintain connection with newfound friends on the other side of the globe. I had not thought to ask about these factors in our initial intake. Her symptoms existed between these truths. By resisting reductive bias, I can allow patients to share their entire story, unhindered by our mutual desires for causal attribution. A singular cause need not always be uncovered at the first visit. It became apparent that I could be of greatest utility, sometimes, by simply being present and listening. Leaving an open differential early on can plant seeds for more tailored care as the clinician–patient relationship develops.”
She closes by mulling her role as a clinician. “Communicating with my patients is not only about extracting the ‘correct’ diagnosis or delivering the ‘ultimate’ treatment. It is about collaboratively constructing meaning, with narrative humility that allows for ambiguity and complexity in our patients’ lives. Seeking tidy plot lines risks distorting our patients’ stories and our ability to connect with them. My patients’ struggles rarely stem from a single source, and their necessary healing rarely comes from a single intervention. There are neither Chekhov’s guns nor silver bullets in psychiatry.”
A few thoughts:
1. This is a great essay.
2. Who isn’t quick to give a diagnosis early in training?
3. But the richness and nuance of the field are discovered when we move past that.
The full Academic Psychiatry paper can be found here:
https://link.springer.com/article/10.1007/s40596-026-02314-y
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments