From the Editor
Many of us enjoy drinking coffee before a busy afternoon clinic. Is that cup of java actually healthy? Do caffeinated beverages like coffee and tea reduce the risk of dementia?
Smaller studies have suggested that they do reduce risk; a meta-analysis of coffee drinkers had a similar finding. In an impressive, new JAMA paper, Yu Zhang (of Harvard University) and his co-authors attempt to answer these questions. They report on a prospective cohort study involving almost 132 000 people, looking at dementia risk with a follow-up period up to 43 years. They found a reduction of about 18%. “Greater consumption of caffeinated coffee and tea was associated with lower risk of dementia and modestly better cognitive function, with the most pronounced association at moderate intake levels.” We consider the paper and its implications.

A cup (or two) a day keeps the doctor away?
It’s the paradox of modern psychiatry. Our medications and therapies have never been better, yet access remains poor and quality is uneven, in part because there is no mental health “system.” So, what can be done? In the second selection, from the podcast series Quick Takes, I sit down with Dr. Paul Kurdyak. In addition to being the longest serving ED psychiatrist at CAMH, he is the Vice-President, Medical, of Ontario Health’s Mental Health and Addictions Centre of Excellence. “Good systems just work. They don’t need to be navigated.”
And in the third selection, Madeline Till, a psychotherapist, writes about the struggles of her son, who has schizophrenia. In a New York Times essay, she wonders whether it would be easier if he had cancer. “More than anything else I have ever wanted, I want to stop this revolving door. I want schizophrenia to be treated with the same urgency, seriousness and continuity as any other life-threatening illness.”
DG
Selection 1: “Coffee and Tea Intake, Dementia Risk, and Cognitive Function”
Yu Zhang, Yuxi Liu, Yanping Li, et al.
JAMA, 9 February 2026 Online First
Alzheimer disease (AD), the most common cause of dementia, currently affects more than 6 million people in the US, and is projected to nearly double to 13 million by 2050. The clinical trajectory of dementia is often conceptualized as a continuum that may begin with subjective cognitive decline (a stage where individuals report perceived cognitive changes), progressing to mild cognitive impairment with measurable deficits on objective cognitive testing, and ultimately to clinical dementia.
With limited treatment options and potential adverse effects of available therapies, early prevention is crucial. Among modifiable risk factors, dietary components have garnered increasing attention. Coffee contains bioactive compounds, including caffeine and polyphenols, which may offer neuroprotection by reducing oxidative stress and neuroinflammation. Experimental studies suggest that chronic caffeine exposure may influence AD-related processes, including amyloid and tau pathways, and AD pathogenesis is increasingly recognized as multifactorial, involving additional mechanisms such as lysosomal or autophagy dysfunction and neuroinflammatory or immune responses…
Several prospective studies have examined coffee and caffeine intake with cognitive health, yet findings remain inconsistent. Notably, the dose-response relationship between caffeine intake and cognitive decline or dementia risk varies across studies; some studies suggested increased risk at higher intake levels, whereas other studies indicated protective effects that stabilize at higher intake levels. Most previous studies were limited by single dietary assessments and short follow-up periods, making it difficult to evaluate long-term effects on cognitive outcomes.
So begins a paper by Zhang et al.
Here’s what they did:
- They drew on two prospective cohort studies that included female participants from the Nurses’ Health Study (data from 1980-2023) and male participants from the Health Professionals Follow-up Study (data from 1986-2023).
- People were excluded who had a history of cancer, Parkinson disease, or dementia at baseline.
- “Dietary intake was measured using validated semiquantitative food frequency questionnaires (FFQs) that were administered at baseline and every 2 to 4 years thereafter.”
- The primary outcome: dementia, which was identified via death records and physician diagnoses.
- Different statistical analyses were done, including modeling coffee, tea, and caffeine intake as time-dependent covariates.
Here’s what they found:
- There were 131 821 participants.
- Demographics. The mean age was 46.2 years (NHS cohort) and 53.8 years (HPFS cohort); 65.7% were female.
- Dementia. During up to 43 years of follow-up (with a median of 36.8 years), there were 11 033 cases of incident dementia.
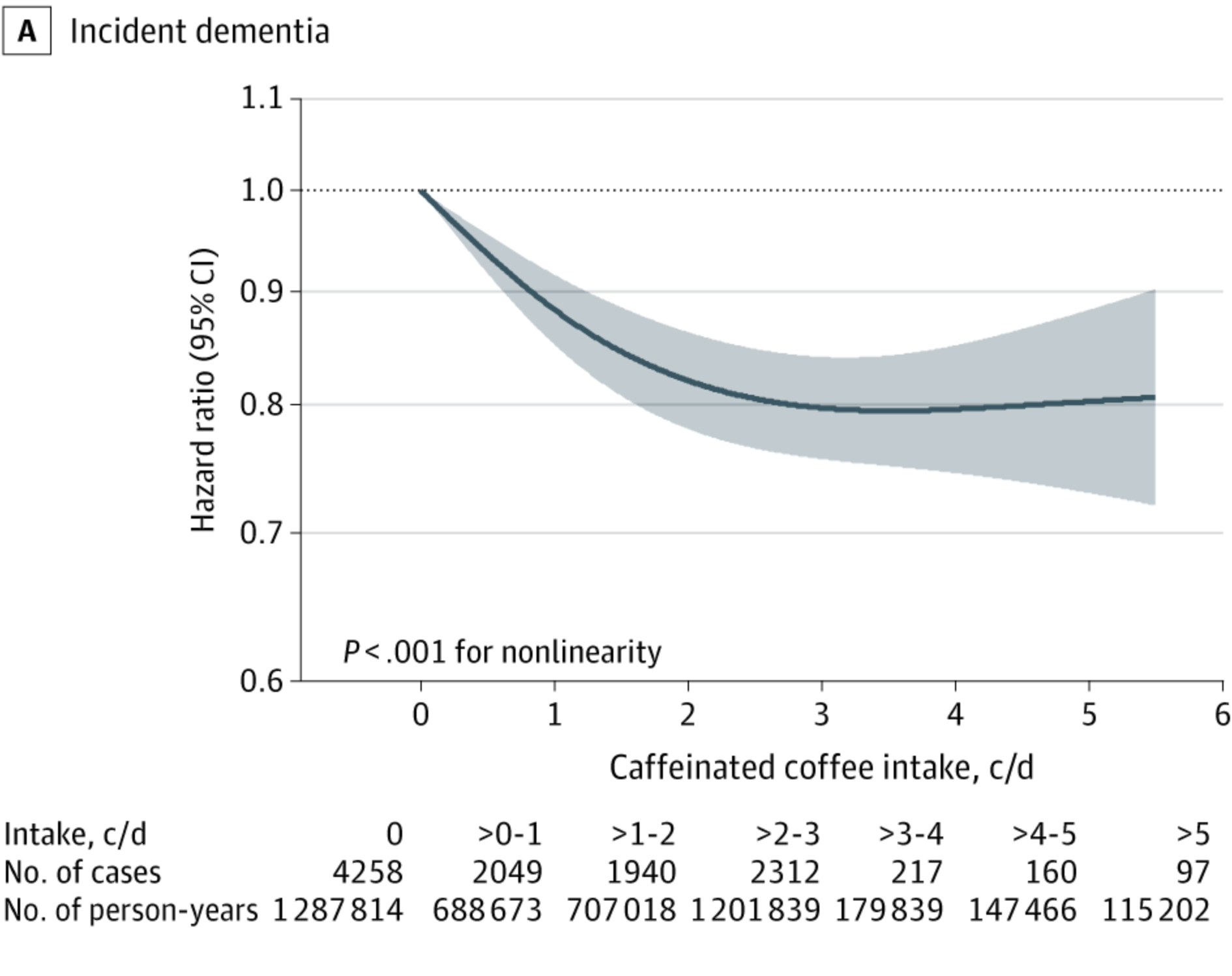
- Caffeine intake. “After the 2 cohorts were pooled, the incidence rate of dementia was 330 per 100 000 person-years for the first quartile (lowest intake) of caffeinated coffee intake, 298 per 100 000 person-years for the second quartile, 229 per 100 000 person-years for the third quartile, and 141 per 100 000 person-years for the fourth quartile.”
- Analyses. “In the multivariable-adjusted analyses, a higher level of caffeinated coffee intake was associated with a lower risk of dementia. Compared with the first quartile (lowest intake) of caffeinated coffee intake, the pooled HR for dementia was 0.98… for the second quartile, 0.81… for the third quartile, and 0.82… for the fourth quartile.”
- Dose-response. “Consumption of approximately 2 to 3 cups per day of caffeinated coffee, 1 to 2 cups per day of tea, or 300 mg/d of caffeine was associated with the lowest risk of dementia compared with no consumption; greater differences were not observed at higher intake levels…”
A few thoughts:
1. This is an important study, drawing on a big dataset with a long follow-up period, published in a major journal.
2. The main finding in a sentence: “higher intake levels for caffeinated coffee, tea, and caffeine were associated with a reduced risk of dementia.” To add a bit more detail: drinking of caffeinated coffee and tea bestowed the advantage (moderate consumption was about 18% lower risk), but not decaf.
3. Wow.
4. How to understand the result? The authors write about several potential mechanisms of action. “Caffeine may lower brain proinflammatory cytokines and mitigate neuroinflammation, which are key contributors to cognitive decline and the development of AD.” The key, though, is the caffeine. After all, those who drank decaf coffee and tea didn’t have a reduced risk (a strike against the argument that antioxidants, not caffeine, make the difference). It’s also interesting to note that there was a sweet spot; moderate use was superior to a cup a day of coffee or four cups a day.
5. Like all studies, there are limitations. The authors note several, including: “reverse causation cannot be fully excluded because early or prodromal cognitive changes may influence beverage consumption patterns or reduce the accuracy of self-reported dietary intake.” It should be noted that the participants were all in healthcare and thus not representative of the general population.
6. And, of course, there are practical considerations. (If I drank three cups of coffee a day, I would never sleep…)
The full JAMA paper can be found here:
https://jamanetwork.com/journals/jama/article-abstract/2844764
Selection 2: “Building a Better Mental Healthcare System”
Paul Kurdyak
Quick Takes, 18 February 2026

In this episode of Quick Takes, I speak with Dr. Kurdyak. We discuss the differences between mental healthcare and other areas of healthcare. We explore the importance of measurement-based care. And we talk about the need for more accountability and incentives, drawing on his Ontario experiences.
Here, I highlight several comments:
On working in an ED as a psychiatrist
“I’ve always loved the work in the emergency department. I’ve always liked the acute stuff.
“What I like about our emergency department is the fact that it is an open door in a sector that has a lot of cliffs and walls. What I don’t like about the work is that it is so rare for something like the CAMH emergency department to exist.”
On experiencing cancer care with a family member
“We went to Clinic A. There was a red digital sign above Clinic A that said we apologize – Clinic A is running two minutes behind. We got called in at 10:27…
“What a difference, working and studying our sector and then having this real-world experience of this other area of our healthcare system that’s so phenomenally different in terms of access, standardization, transparency, accountability, and the ability to monitor performance for greater good.”
On diabetes and depression
“Depression is a little bit like hypertension or diabetes. In our healthcare system, there’s an understanding that primary care is going to do first-line care for diabetes. And most people are going to respond to that first-line care. But if people don’t respond to the first-line care – they seem to be treatment refractory – those the individuals for whom the specialists, like the endocrinologists, are better suited to help support primary care to manage.
“In depression care currently, half the people get nothing; some people get antidepressants prescribed to them in primary care, but it’s not measurement based and it’s usually not evidence based in the sense that it’s usually not adequate dosage and duration. There’s no measurement about whether people respond to the care they’re given.”
On how the system would look a decade from now for a person with depression who isn’t responding to medications
“Ten years from now, he’d never come to the ED. That’s just not an ED case, right? He’d get measurement-based, evidence-based care. He’d get psychotherapy plus pharmacotherapy. And then there would just be an evidence-based and measurement-based care pathway that gets him what he needs. The ED will look very different in ten years. We’re going to have regional coordinated access where all the services are behind one door. Primary care physicians can do what they can, but then once they can’t, they refer people to this one door.”
The above answers have been edited for length.

The podcast can be found here, and is just over 30 minutes long:
Selection 3: “Why Is My Son Being Left to Die on the Streets?”
Madeline Till
The New York Times, 28 January 2026

My husband and I adopted our son, Abraham, as a toddler, believing we could provide him with a good life. Abi, as we called him, was a bright, curious kid who blossomed into a kind and popular teenager, a star student who won a scholarship to the University of Michigan. In his last year of high school, though, he began acting in ways we could not understand.
Abi tore family photographs from the walls and burned them in what he called a ‘death ritual.’ He announced that he was a prophet of God. He stole our cars. Two of our other children were living at home, and all of us woke up every day terrified to find out what had happened in our home overnight. Abi was diagnosed with schizophrenia, but as is often the case, he was unable to perceive that he was ill. Nothing – not psychiatric care, not even police intervention – could convince him he needed help. Then he turned 18. He became an adult in the eyes of the state, and that was the end of our influence.
Now, three years later, Abi drifts from parking garages to homeless shelters, panhandling on sidewalks for a few coins. He won’t come home; he won’t even stop by for food or medicine.
So begins an essay by Till.
She notes the cycle of hospitalizations and discharges. “Every few months, he acts out more than usual and he is hospitalized. Doctors administer enough medication to briefly calm him, then label him ‘stable’ and ‘not a harm to self or others’ and discharge him back to the streets, where he is exposed to harsh winter nights without any support – sometimes even without shoes or a jacket.”
She wonders if it were better if he had cancer. “I know that sounds crazy, and of course it is. As a psychotherapist, I sit with families every day whose children face illness, pain and death. I lost my beautiful 7-year-old niece to a brain-stem tumor. I understand the weight of a cancer diagnosis and I wouldn’t actually wish it on anyone, certainly not my own child. But I have seen how people respond to cancer: with urgency, empathy and effort. When someone has cancer, there are people to turn to, people who really try to help. When the daughter of a woman I know finished treatment, the hospital staff gathered to watch as she rang a bell they keep on hand for such occasions, and everyone erupted into applause.
“There is no bell for mentally ill individuals marking their survival through another brutal season of homelessness, wandering the streets untreated, unsheltered and utterly vulnerable.”
She describes a revolving door of care. “Since Jan. 1, 2024, Abi has been in hospital emergency rooms at least 20 times. Sometimes we hear about it in time to steel our hearts and go see him. We know that he will have been medicated, and might even be lucid, but we also know that he will soon be discharged – with prescriptions he cannot fill, appointments he cannot organize and instructions he cannot follow – and we will lose him again.”
She details her frustrations with the system – hospital administrators and physicians who don’t respond to emails because of her son’s privacy; police officers who seem indifferent. “Some angels do emerge, typically those with the least power. Immigrant shop owners offer our son food or clothing. They often express dismay that this country treats mental illness so poorly. They tell me to send him back to Ethiopia, where we adopted him, because he’ll get better support there.”
Where should we go? “We do not need to return to the large, abusive psychiatric asylums of the past, but the law has swung so far toward individual autonomy that the concept of ‘do no harm’ has all but vanished. If someone is so severely ill that he clearly cannot care for himself, it should be possible for him to be committed. And once committed, it should be possible for him to get actual care, rather than being pushed back out the door by an insurance system that rewards brief stabilization over comprehensive long-term treatment. Being left to die on the street is not freedom.”
“I want my son’s life to be treated as though it is worth saving.”
A few thoughts:
1. This is a moving essay.
2. It’s tough not to feel for her son – yes – but also her and her husband. Schizophrenia is a diagnosis for one person but it affects a family.
3. Is she right about changing the legal framework? Readers can draw their own conclusions. Increasingly, politicians find this argument persuasive.
The full NYT essay can be found here:
https://www.nytimes.com/2026/01/28/opinion/family-mental-health-homeless-schizophrenia.html
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments