From the Editor
Imagine the excitement if a new antidepressant came to market that boasted that it could achieve the symptom reduction of other antidepressants in about half the time, yet had no significant new side effects.
There is no new antidepressant, but there is a study to mull: In 2015, The American Journal of Psychiatry published a paper on measurement-based care for people with depression, and the patients in the measurement group achieved remission in about half the time compared to people seeing a psychiatrist without the guidance of measurement. Though the paper has limitations, it also suggests the incredible potential of measurement-based care.
In the first selection, we consider a new review paper published in JAMA Psychiatry. Kaiser Permanente Washington Health Research Institute’s Cara C. Lewis and her co-authors contemplate the potential of measurement-based care – and its reality (greatly underused). They make six points of observation and discussion before going on to propose an agenda.
In the second selection, we look at a paper by the University of Pennsylvania’s David W. Oslin and his co-authors who use survey data to consider the use of measurement-based care in a paper published by Psychiatric Services.
DG
Better Care and Big Obstacles
“Implementing Measurement-Based Care in Behavioral Health: A Review”
Cara C. Lewis, Meredith Boyd, Ajeng Puspitasari, Elena Navarro, Jacqueline Howard, Hannah Kassab, Mira Hoffman, Kelli Scott, Aaron Lyon, Susan Douglas, Greg Simon, Kurt Kroenke
JAMA Psychiatry, 19 December 2018 Online First
https://jamanetwork.com/journals/jamapsychiatry/article-abstract/2718629
Depression and other behavioral health disorders are increasing in the United States and worldwide. Evidence suggests that measurement-based care (MBC) or the use of patient-reported outcomes (PROs) to identify the extent of these problems and inform treatment decisions can improve usual care for these conditions. However, it is underused; less than 20% of practitioners (17.9% of psychiatrists, 11.1% of psychologists, and 13.9% of masters-level practitioners) engage in MBC, and as little as 5% use it according to its empirically informed schedule (ie, every session). These rates reflect the status quo in the United States, the United Kingdom, and Australia despite policies recommending PRO use.
Numerous reviews and meta-analyses have summarized the evidence base for MBC, with a recent article highlighting MBC delivery in pragmatic trials and suggesting that its scale-up and spread is needed. However, no reviews, to our knowledge, have sufficiently summarized the barriers to using MBC in routine care and the strategies needed to implement MBC with fidelity. This narrative review addresses definitional issues, describes a concrete and evaluable operationalization of MBC fidelity, and summarizes the evidence base and utility of MBC. The review also synthesizes the extant literature’s characterization of barriers to MBC and strategies for supporting its implementation, sustainment, and scale-up and summarizes the learnings from the review in a 10-point research agenda to improve the integration of MBC in routine care into clinical practice.
 Cara C. Lewis
Cara C. Lewis
So begins a paper by Lewis et al.
In it, Lewis and her co-authors consider six observations and points of discussion.
Operationalization of MBC Fidelity
While the authors see four core elements of measurement-based care – some type of process measure, practitioner review of data, patient review of data, and collaborative re-evaluation of the treatment plan informed by data – they note a lack of agreement on basic terms and core components. “This evidence-based practice is referred to in at least 16 different ways in the literature with no discernable preference for terms across 17 countries…”
They suggest that: “The field would benefit from harmonization of terms and operationalization of core components to promote efforts to monitor MBC fidelity.”
Mechanisms of Action for MBC
There is no one mechanism of action, obviously. That said, the authors note that in psychopharmacology practice: “Measurement-based care seems to inform more rapid dosage increases and hasten the rate at which practitioners change medications, which in 1 study led to a faster rate of recovery and a higher rate of response.” For psychotherapy practice, there is no medication algorithm but there are options for “consultation with supervisor, revising case conceptualization, changing session focus, increasing session frequency, and adding services.” The authors also see a patient connection in terms of a mechanism of action. “Patient expectation of gains, therapeutic alliance, and enhanced accuracy of practitioner understanding of patient improvement are hypothesized MBC mechanisms of action that require additional investigation.”
Effectiveness of MBC Over Usual Care
The authors review the literature, finding: “At least 9 review articles state that MBC outperforms usual care, with significantly improved outcomes, particularly for patients deemed to be nonresponders, often reflective of medium to large (eg, 0.22-0.70) effect sizes. Measurement-based care is associated with decreased likelihood of patient deterioration while in treatment and costs of care. Youth who receive MBC have demonstrated faster symptom improvement.”
They review 21 randomized clinical trials, noting: “Measurement-based care can be conceptualized as a transdiagnostic and transtheoretical practice.” They caution, however, that a Cochrane review had found the “evidence to date was low quality…”
Utility of MBC Across Stakeholder Levels
They note the benefits of measurement-based care for many involved in health care:
Measurement-based care offers benefits across multiple levels: patients, practitioners, and organizations. For patients, MBC encourages active involvement in the treatment process, helps patients better understand their symptoms, and allows patients to more easily quantify and communicate their experience. For practitioners, MBC alerts them to patient lack of progress, which is important given evidence that practitioners typically overestimate how well patients are doing in treatment. Measurement-based care can direct practitioners to recognize important treatment targets (eg, sleep, suicidality), observe factors associated with change, facilitate care coordination or collaboration (between practitioners and the treatment team), and inform treatment decisions (eg, need for adjunctive services, increased dose)…
Barriers to MBC Implementation
“Measurement-based care is underused worldwide.”
They see a variety of barriers. For example, for patients, there may be response burden and concerns around confidentiality. For providers, “increased time, effort, and cost,” as well as negative attitudes toward MBC.
Strategies to Implement MBC
The authors consider various challenges to implementation, and offer suggestions.
I highlight a few:
- “Careful thought should be given to the measures used and the method of administration.”
- “Measures chosen should assess the domains most relevant to various stakeholders (eg, patients, practitioners, administrators, and funding bodies) and should be low burden for respondents (ideally taking only a few minutes to complete) and those scoring and interpreting the measure.”
- “Measure scores should be sensitive to patient change over time, which can inform response from practitioners.”
- They also emphasize the importance of “identifying and leveraging local champions.”
They conclude with a ten-point agenda:
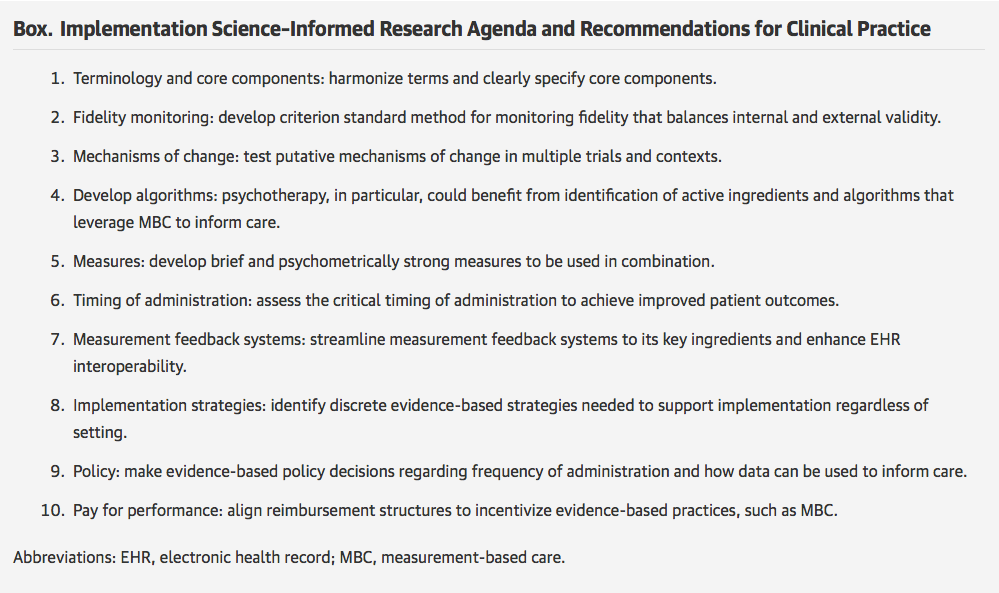
Despite decades of research affirming MBC as an evidence-based practice capable of improving patient behavioral health outcomes, several empirical gaps remain. This narrative review informed a 10-point agenda aimed to address practical, clinical questions that will support MBC use. Recommended points emphasize the need for research on MBC in the context of psychotherapy given that less work has been completed in this area in comparison with pharmacotherapy.
A few thoughts:
- This is a good review paper.
- The paper was published in JAMA Psychiatry – a journal that frankly hasn’t published much in this area historically. Is this something of a turning point for measurement-based care?
- The statistics cited are striking. Measurement-based care is infrequently used by psychiatrists, and – even when they do it – they often don’t use it regularly. Ouch.
- That said, it’s difficult not to feel a bit optimistic reading this paper.
- We opened by talking about Guo et al.’s paper in The American Journal of Psychiatry. It’s worth returning to that paper, which is referenced more than once by Lewis et al. Guo and his co-authors found much better results for the measurement-based care group: Patients responded better than the standard treatment group (86.9% vs. 62.7%); they had a much higher remission rate (73.8% vs. 28.8%); their time to response to treatment was shorter (4.5 weeks vs. 8.1 weeks). Here’s a graphical summary from the study:

(That paper was considered in an earlier Reading, which you can find here: http://davidgratzer.com/reading-of-the-week/reading-of-the-week-depression-and-measurement-based-care-depression-week-1-of-3/.)
- How do different types of providers use and view measurement-based care? The next selection seeks to answer that question.
Better Care and Provider Views
“Provider Attitudes and Experience With Measurement-Based Mental Health Care in the VA Implementation Project”
David W. Oslin, Rani Hoff, Joseph Mignogna, Sandra G. Resnick
Psychiatric Services, 30 October 2018 Published Online
https://ps.psychiatryonline.org/doi/10.1176/appi.ps.201800228
The paper opens by noting that the concept of measurement-based care “is paramount to treating chronic conditions such as diabetes or hypertension, but it is not commonplace in mental health care and is not well understood by many mental health clinicians.” They note the approach is associated with better outcomes and better patient satisfaction. But how common is measurement-based care used and what are provider attitudes about it? The authors sought to answer these questions with a survey of providers working in the U.S. Department of Veterans Affairs.
Here’s what they did:
- They distributed a survey of 32 questions to gauge provider knowledge and attitudes to measurement-based care.
- They found a local champion in each of the 58 sites of the VA, who was then asked to distribute the survey locally.
- Measurement-based care was defined as “repeated use (two or more occasions) of the same patient-reported outcome measure within the first 6 months of a new episode of care.” Scales that needed to be used included the Patient Health Questionnaire-9 (PHQ-9).
Here’s what they found:
- 296 surveys were returnedbut some data was excluded. They analyzed the data from 230 providers, including 26 psychiatrists, 23 nurses, 135 psychologists, and 46 social workers.
- “More than half of the providers (58%) reported collecting at least one measure for at least half of their patients.”
- “Nearly half (44%) reported collecting measures repeatedly during an episode of care.”
- “Providers frequently shared the results of outcome measures with patients, with 72% indicating that they usually or always explained the results to patients and 65% indicating that they used the results as part of shared decision making.”
- But results varied significantly by discipline. Only 16% of psychiatrists reported collecting at least one measure for at least half of their patients. (That percentage was higher for everyone else: 44% of nurses, 57% of social workers, and 71% of psychologists.) And only 8% of psychiatrists reported collecting measures repeatedly for at least half of their patients. (Again, higher for other disciplines: 30% of nurses, 44% of social workers, and 54% of psychologists.)
They conclude:
The results of this survey are encouraging, but they also point to a needed cultural shift in the way mental health care is delivered. Providers expressed favorable attitudes for using measures in clinical practice, but these attitudes varied significantly by discipline.
- Their opening comment is worth repeating. The concept of measurement-based care “is paramount to treating chronic conditions such as diabetes or hypertension, but it is not commonplace in mental health care and is not well understood by many mental health clinicians.”
- The survey gives us some data, though there are clear limitations to the approach, including the reliance on champions who were already involved in measurement-based care (thereby creating a selection bias).
- Psychiatrists were the least likely of any type of provider to use measurement-based care. Ouch.
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments