From the Editor
He spoke about depression and its impact on his life but held back on certain details. Only when his family showed me the texts did I fully understand how ill he really was.
Patients often conceal some aspects of their problems. In a new paper published in the Journal of Medical Internet Research, Chloe Roske (of the Albert Einstein College of Medicine) and her co-authors shed light on this concealment with a creative approach: by analyzing social media. Drawing on nearly 100 TikTok videos with more than 73 million views, they conducted a qualitative analysis. “TikTok creators frequently described concealment as a strategy to avoid perceived punitive consequences, manage interpersonal dynamics, or cope with emotional distress.” We consider the paper and its implications.

In the second selection, Benedikt Fischer (of Simon Fraser University) and his co-authors discuss Canada’s legalization of cannabis, noting a decline in crime but an increase in problematic use. “Nonmedical cannabis legalization in Canada was a milestone policy reform when implemented almost a decade ago. However, complacency about its presently main outcomes would be misplaced, also since its original objectives have been at best partially achieved.”
And, in the third selection, Dr. Stefani Mihilli (of the University of Toronto) and her co-authors discuss antidepressants in a paper for The Canadian Journal of Psychiatry. They focus on the commonly made claim that antidepressants take several weeks to start working. “Telling patients that antidepressants ‘kick in’ after 2–4 weeks is not only potentially inaccurate but also may cause unnecessary distress or even reduce positive outcomes.”
DG
Selection 1: “Why People Conceal Mental Health Problems: Qualitative Analysis of TikTok Posts”
Chloe Roske, Kael Ragnini, Qinchun Zhu, et al.
Journal of Medical Internet Research, 19 May 2026
Approximately 50% of people in the United States are diagnosed with a psychiatric disorder during their lifetime, yet few seek mental health treatment. Of those who do, many conceal the extent and existence of symptoms from clinicians, which limits the delivery of adequate treatment. Concealment has been associated with worse therapeutic outcomes and may be most consequential for patients with suicidal thoughts and behaviors (STBs). If a clinician is unaware of a patient’s suicidal thoughts or intent, they may not provide evidence-based treatments for STBs and ultimately be unable to intervene to prevent death by suicide… Around 90% of people conceal significant information from their clinicians, with that information most frequently being about STBs. A study of psychiatric inpatients showed that 51.5% withheld some information about SI during admission…
To date, research on concealment of STBs has relied on self-report and interview-based methods conducted in research settings… Social media may offer more naturalistic insight into reasons why patients conceal information from their treatment teams. People often turn to social media when seeking peer support for psychiatric and nonpsychiatric illnesses and engaging in discourse about mental health. TikTok, a platform for sharing short-form videos, has recently begun to dominate the social media landscape… As a result, TikTok hosts a vast collection of new, user-generated content on subjects ranging from eating disorder treatment to discussion of mental health symptoms…
Here’s what they did:
- The authors created a TikTok account (thus minimizing algorithmic bias), and identified and downloaded the 25 most-viewed English-language videos from four search terms related to concealment in clinical contexts (including “lying to doctors about mental health”).
- After exclusions, 98 videos were included in the analysis.
- “Videos were analyzed using reflexive thematic analysis. Four coders collaboratively developed a codebook through iterative review, triangulation, and consensus discussions.” The process involved videos being watched and re-watched, a group debrief, and the development of a codebook draft.
- “Engagement metrics (views, likes, comments, shares, saves) were recorded and summarized.”
Here’s what they found:
- The 98 videos received 73 252 531 views and more than 14 million likes.
- Themes. Four themes were identified: (1) disclosure perceived as punitive (34.4% of videos), including desire to avoid hospitalization (18.8%); (2) managing others’ feelings and impressions (31.1%), including fear of upsetting therapists (5.5%) and maintaining a façade of wellness (7.7%); (3) negative emotions or inability to identify feelings (23.3%), including fear of vulnerability (6.6%); and (4) negative opinions of psychiatric treatment (18.8%), including concerns about confidentiality (3.3%).
- Focus on the second theme (managing others’ feelings and impressions). “Videos with this theme discussed how other people factored into their decision-making about disclosure. Eleven videos specifically talked about parents and family. Some creators considered other people’s emotional responses to their symptom disclosure when deciding whether to report or conceal their symptoms… One video is a cartoon depicting a creator’s experience disclosing to their therapist who ‘cri[ed] after hearing [their] story for the first time.’ As a result, the creator says that they felt ‘guilty immediately’ and felt ‘bad for making them cry and stop[ped] talking completely.’”
- Exploratory theme. “An exploratory theme captured ambivalence and guilt surrounding nondisclosure.”
A few thoughts:
1. This is an interesting study.
2. The main finding: “Thematic analysis of naturalistic, user-generated social media content suggests that concealment of psychiatric symptoms is often motivated by fear of punitive consequences, stigma, interpersonal dynamics (within family, treatment team, and one’s broader social context), and dissatisfaction with treatment practices…”
3. There is something new and fresh about this study, tapping a data source (social media) that isn’t typically used in such studies. For the record, the number of views of the TikTok videos is striking.
4. That said, is there anything particularly surprising in the findings?
5. In some ways, is the idea of this study more exciting than the study itself? Still, looking to social media is new and fresh.
6. Of course, there are clear limitations here. The authors note several, including “the specific symptoms that patients were concealing were sometimes unknown.”
The full JMIR paper can be found here:
https://jmir.org/2026/1/e88244
Selection 2: “Cannabis Legalization Outcomes in Canada: Trading Off Increased Health Problem for Reduced Crime Burdens Is Not Good Enough”
Benedikt Fischer, Wayne Hall, Didier Jutras-Aswad, et al.
The Canadian Journal of Psychiatry, 20 May 2026 Online First

In 2018, Canada was the first G-20 nation to undertake major liberalization of its cannabis policy by implementing the legalization of nonmedical cannabis use and supply for legal-age adults, including commercial, regulated cannabis production, and retail systems. The aims of the legalization policy were to improve cannabis-related public health outcomes, prevent cannabis use among youth, and reduce cannabis crime and illicit market. The federal Cannabis Act set the central legal framework for minimum standards, while allowing variations in provincial/territorial regulations for key parameters (e.g., regarding legal use age, retail distribution models, home-growing, places of use) and so creating a heterogeneous patchwork of regulatory sub-systems across the provinces and territories. By 2024/2025, there were some 3,700 licensed cannabis retailers and 1,000 cultivators/producers, with an annual sales volume of $5.5 billion…
So begins a paper by Fischer et al.
“Some 26–32% of Canadian general population adults are currently active (i.e., past 12 months) cannabis users, thus pointing to substantial increases in the prevalence of cannabis use associated with legalization compared with prior periods.” (!)
They note other aspects of use:
- Youth. “The prevalence of cannabis use among youth… has steadily stood at substantially higher levels of 40% or above.”
- Daily use. “About one-in-four (25%) of active cannabis consumers use cannabis on a daily/near-daily basis – an intensive use pattern that commonly involves high-potency products and that is strongly associated with various – acute and chronic – cannabis-related harms (e.g., cannabis use disorder, mental health problems).”
- Driving. “As many as 20–24% of active (past-year) cannabis users have reported driving a motor-vehicle immediately after consuming (e.g., smoking/ingesting) cannabis products, a leading cause of cannabis-related injury and/or death due to impairment.”
They note, though, a reduction in crime. “While there were some 70,000 police-recorded cannabis offenses – mostly for personal possession – in 2014 just prior to legalization, this annual number of enforced cannabis incidents has vastly dropped to 8,879 offenses (with only a small proportion [13%] for possession) in 2024 and so markedly reduced the cannabis-related enforcement burden.”
Thus, they describe a mixed picture. “There have been marked increases in cannabis use prevalence and cannabis-related health problem outcomes associated with legalization… At the same time, the majority of legal-age cannabis consumers are now obtaining their cannabis products from legal/licensed sources, so avoiding involvement with and sustaining illicit cannabis markets. Related, the extensive burden of – mostly user-focused – cannabis enforcement and criminalization that existed before legalization has been vastly reduced, averting tens-of-thousands of cannabis-related arrests and related adverse consequences of personal, professional, and social hardship that would have been expected in its absence.”
They ask a question of policy makers. “Is this rather mixed outcome picture of marked increases in cannabis use and related health problems, and decreases in cannabis use-related crime and enforcement generally acceptable for legalization as the chosen policy reform option for cannabis control in Canada?”
They argue that it isn’t and point a way forward. “There are multiple evidence-based policy and regulation levers available for utilization by policy-makers especially to reduce the current burden of adverse health outcomes to ensure that cannabis legalization equally and effectively serves to reduce both related health- and crime burdens in Canada.”
They outline several ideas.
Targeting high-potency cannabis
“Extensive amounts of cannabis consumption now involve high-potency/strength cannabis products (e.g., >20% THC) associated with elevated risk for adverse health outcomes (e.g., psychosis, CUD), especially for vulnerable (e.g., youth) consumers that should be subject to age-appropriate education and consideration of access restrictions.”
Focusing on youth
“Cannabis use levels among underage youth – a subpopulation for whom cannabis access is illegal and was to be reduced through legalization – remain unacceptably high. Improved interventions, including better use prevention and efforts to curtail common (e.g., social) cannabis sourcing routes, appear required.”
Reigning in industry
“There are signs of ‘commercialization creep’ among cannabis production/retail sectors, including commonplace violations of regulatory restrictions on cannabis advertising/promotion supposed to protect vulnerable (e.g., underage) groups from inducements. Yet, the cannabis industry has lobbied to further relax related restrictions.”
A few thoughts:
1. This is an excellent commentary, offering data, solid analysis, and practical policy ideas.
2. Regardless of whether you approve or disapprove of the legalization, their suggestions are relevant and thoughtful.
3. Should Canadians be content with less crime but higher use?
The full Canadian Journal of Psychiatry commentary can be found here:
https://journals.sagepub.com/doi/10.1177/07067437261448740
Selection 3: “When Do Antidepressants ‘Kick In’: Addressing the 2–4-Week Myth”
Stefani Mihilli, Anthony Levitt, Marco Solmi, et al.
The Canadian Journal of Psychiatry, 7 May 2026 Online First
Treatment guidelines for major depressive disorder (MDD) recommend pharmacotherapy as the first-line treatment for many patients with depression. Prior to initiating treatment with an antidepressant medication, patients are counselled regarding the expected onset of clinical improvement. Yet, there is a substantial mismatch between published recommendations surrounding what to tell patients and the precise interpretation of evidence regarding the time to onset of antidepressants. According to the American Psychiatric Association guidelines (2010), it may take 2–4 weeks before patients may notice the beneficial effects of pharmacotherapy.
So begins a paper by Mihilli et al.
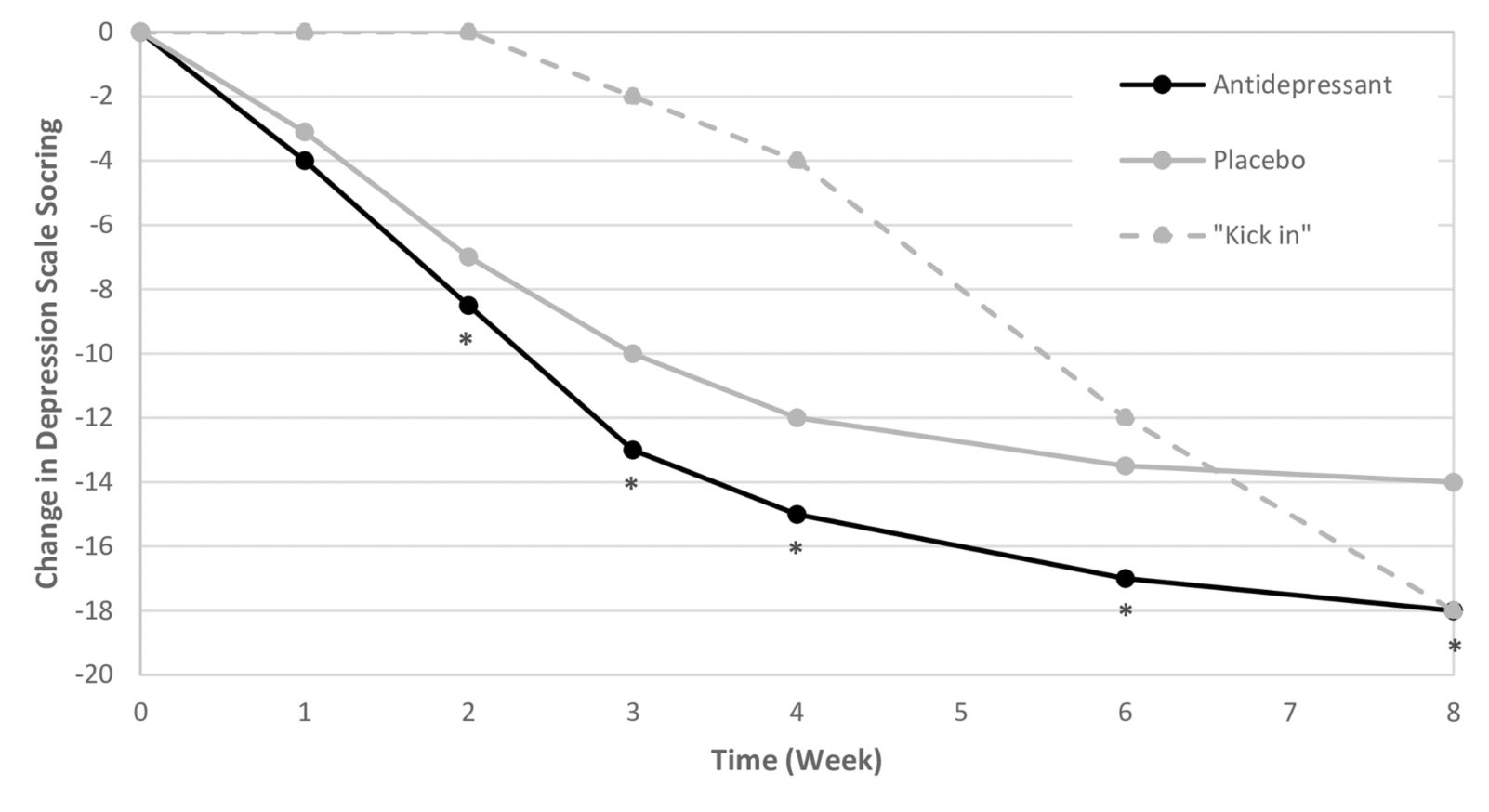
“Randomized controlled trials (RCTs) that investigate the onset of antidepressant action reveal improvements over time that generally resemble illustrative Figure 1 (see below). This is a conceptual figure created to reflect typical results from placebo-controlled RCTs in MDD investigating clinical improvement with antidepressants. In general, clinical improvement that is measured through a validated scale may enhance identification of early improvement, and more data is needed during these early stages to better characterize the specific course of early antidepressant response. In these studies, the onset of action is often reported as the time at which the antidepressant arm reaches a statistically significant difference from the placebo arm. In further examining these data, the figure highlights that the first 2 weeks of active antidepressant treatment are when the greatest rate of change on the depression rating scale occurs, with change reaching a plateau around the 6- to 8-week mark. Clinically, this means that, in general, patients may experience the most rapid improvement in their depressive symptoms early in the treatment course.”
Further evidence? They describe a meta-analysis, which “reported that one third of the total symptomatic improvement observed with SSRIs during 6-week treatment was observed within the first week.” They argue that the problem is a “misinterpretation” of the clinical trial findings. “This misinterpretation focuses on the time period in which a statistically significant difference emerges in the symptom reduction between the active treatment and placebo arms. This time point is highly germane when establishing group differences in clinical trials, but not necessarily at the individual patient level. From the perspective of an RCT that is aiming to establish whether an active treatment is efficacious, the timing of the appearance of a statistically significant delta between antidepressant and placebo arms is a key metric of interest. Regulatory trials are typically 4 to 6 weeks in length, which makes sense, since this is the period in which a significant separation is typically observed.”
They add: “What patients wish to know is, ‘When will I start to feel better?’ Clinically, the focus is on the patient’s experience of improvement over time, which is fundamentally distinct from a statistical finding indicating separation of active treatment from placebo. From a patient experience perspective, therefore, the most salient information from an RCT is the trajectory of change within the antidepressant arm.”
They see a major problem with advice given to patients. “There is strong evidence that patients’ expectations can partially mediate the effects of antidepressant treatment, and that counselling that is delivered in a way that enhances patient expectations regarding response can be beneficial. As such, by providing information that does not align with the patient experience of the time course of onset, clinicians may inadvertently demoralize patients who are already experiencing a time of great suffering and interfere with positive expectations that often help facilitate a more rapid response.”
A few thoughts:
1. This is a helpful and reasonable paper (part of the Clinician’s Corner series).
2. When patients are carefully observed – say, on an inpatient basis – there is often material improvement in the first two weeks. (That’s been my experience having worked on inpatient units for more than 20 years.)
3. What then to say to patients when starting antidepressants? The authors suggest: “It is very possible that you may begin to notice some improvements in your symptoms soon, even within days, after starting your antidepressant, and that this will build up over time.” Sensible.
The full Canadian Journal of Psychiatry paper can be found here:
https://journals.sagepub.com/doi/10.1177/07067437261448740
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments