A few months ago, a patient walked into my office and immediately broke down. He explained that he had waited so long to see a psychiatrist that he was overwhelmed to finally meet me. For the record, he had never spoken to me before and knew nothing about me – except that I was a psychiatrist and that he needed to see one.
The surprise is that anyone would be surprised by such a story.
Patients often face long wait lists in our health care system. The wait for psychiatric care seems particularly long. But here’s the question: do we have a shortage of psychiatrists in Ontario – or do we have a shortage of creative thinking on how psychiatrists practice in Ontario? The week’s Reading asks this important question, with a surprising conclusion: “increasing psychiatrist supply will have little impact on patients’ access.”
On the Reading of the Week
As we did in January and February, the selection of this week’s Reading was made with the editorial board of the International Psychiatry Twitter Journal Club, allowing us to consider this paper here, and to continue the conversation on Twitter. And that conversation is going on today.

Bonus: the paper’s first author is participating in the Twitter discussion. #VeryNice.
Interested? Follow @psychiatryJC.
On Psychiatric Services
Patients wait for care. It’s difficult to tell how extensive the problem is. “Time to Close the Gap: Report Care on Wait Times in Canada” published by the Wait Time Alliance in 2014 lists benchmark indictors, including for psychiatric care – but there is no data for our specialty. The Wait Time Alliance is a physician-led effort but their dataset simply draws from the provinces, and no province is actively collecting and releasing the psychiatric data.

Last year, Dr. Liisa Jaakkimainen and her co-authors decided to measure wait times for specialist care by looking at the electronic medical records of family physicians. Psychiatry had the second longest waits.
The easy assumption to make is that we simply need more psychiatrists – and that by increasing the supply of these specialists, we will see an increase in the number of patients seen (and ultimately reduce wait times). That’s what makes this Reading so interesting.
On This Week’s Reading
This week’s Reading: “Universal coverage without universal access: a study of psychiatrist supply and practice patterns in Ontario” by Paul Kurdyak et al.
You can find the paper here:
http://www.openmedicine.ca/article/view/624/555
(Because of firewall and browser issues, try cutting and pasting this address directly into your browser if the link doesn’t work.)
Dr. Paul Kurdyak and his co-authors tapped provincial data to shed light on psychiatrists and psychiatric services. The paper has been mentioned numerous times in the media – as recently as this weekend, for example, the Toronto Star referenced the work in an article on a patient trying to find a psychiatrist. There is also been much debate among psychiatrists. At the Canadian Psychiatric Association Annual Meeting last September, Dr. Kurdyak discussed his findings with Dr. Doug Weir (a psychiatrist and past OMA President); the room was full. Next week, here in Toronto, the Ontario Psychiatric Association members will gather – and Drs. Kurdyak and Weir will face off again.
 Dr. Paul Kurdyak
Dr. Paul Kurdyak
Dr. Kurdyak et al. have, in other words, produced a much discussed paper. It’s also an important paper.
Here’s what they did:
· The study authors looked at several databases, including the OHIP database covering physician billings and visits and consultations. (!) In other words, this is a remarkable dataset – though, not fully free of controversy (see below).
· They divided the province by LHINs, with 9 smaller LHINs grouped as a “low-supply” group recognizing the smaller population samples.
· They considered hospital admission data (including a few diagnoses) and follow up data.
· They also looked at practice data – how many outpatients are seen by psychiatrists, including new patients and number of patient visits in a year. (!)
Here’s what they found:
· Regional practice patterns varied dramatically.
· For example, post-discharge follow ups tended to be higher in Toronto Central and Champlain LHINs than in low-supply LHINs.
· The concentration of full time psychiatrists (per 100,000) is highest in the two big urban centres, Ottawa and Toronto.
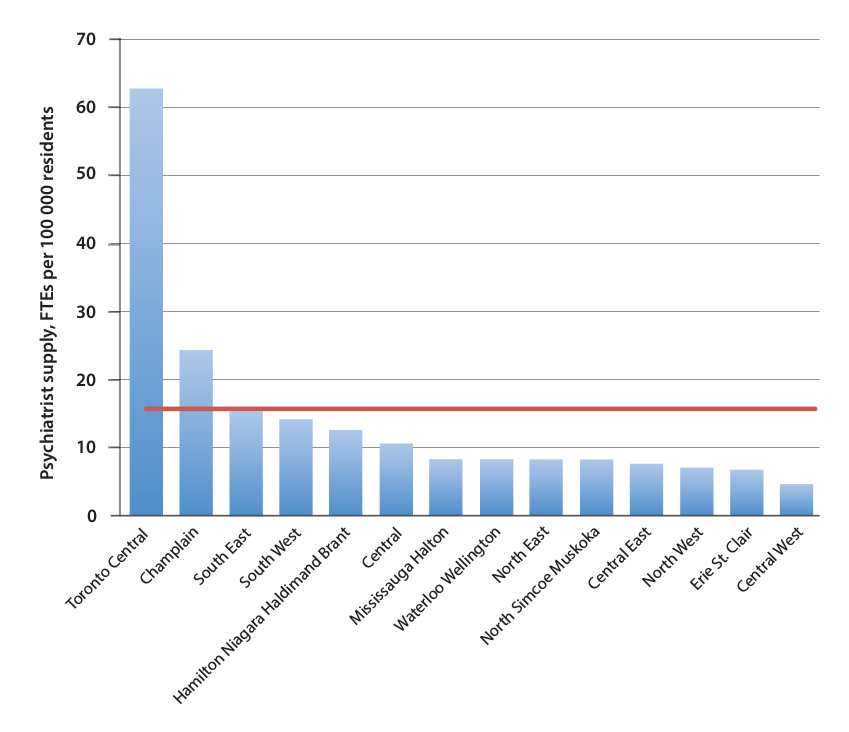
· Outpatient psychiatrist practice patterns vary greatly. But geography yields a somewhat unexpected results: as the supply of psychiatrists increased, the total number of patients that each psychiatrist saw decreased. (!!) They note:
The majority of psychiatrists in all LHINs saw patients, on average, up to 16 times per year, a visit frequency that is consistent with providing consultations, pharmacotherapy, or evidence-based psychotherapy. However, in the high-supply LHINs of Toronto Central, Champlain, and South West, 7%–10% of full-time psychiatrists saw fewer than 40 unique patients per year, compared with less than 4% in the rest of the province. Similarly, 24%–40% of full-time psychiatrists in these high-supply LHINs saw fewer than 100 unique patients per year, compared to less than 15% in the rest of the province.
What makes this paper particularly interesting is the international perspective. Kurdyak et al. don’t simply describe a problem, but then look internationally for possible answers:
In the United Kingdom, Australia, and the United States, the role of a psychiatrist has been modified to prevent this pattern of practice and to improve access to psychiatrists for patients with severe mental illness. In these countries, reimbursement for psychiatric consultations is higher than for psychotherapy, and most psychiatrists in managed care and publicly funded health care settings have stopped providing long-term psychotherapy to a small number of patients. Instead, they have a consultant-based clinical role similar to that of other specialists.
To emphasize the point, the co-authors do a quick review.
U.K. “Psychiatrists have the role of consultants mandated to manage the most complex psychiatric cases, ideally within a multidisciplinary team; the services of psychologists and other mental health workers are covered by public insurance, and these professionals provide evidence-based psychotherapy at a lower hourly rate than the psychiatrists’ consultation rate.”
Australia. “In 2006, psychologists, occupational therapists, and social workers were incorporated into the Australia fee schedule to provide psychotherapy and focused psychological strategies, but they are paid at lower rates than psychiatrist consultation reimbursement. Creating a differential between the relatively high reimbursement for consultations and the relatively low reimbursement for psychotherapy has led to reductions in visit frequency, which suggests that financial incentives were effective in changing psychiatrists’ practice patterns.”
U.S. “Health maintenance organizations have created mental health ‘carve-outs,’ in which psychologists and other allied mental health professionals provide psychotherapy at lower rates, whereas within US Medicaid and Medicare, psychiatrists are paid an hourly fee that is more than twice as high for pharmacotherapy and psychiatric consultations as for psychotherapy.”
As for a conclusion, the study authors don’t mince their words:
Our study confirms, for psychiatric care in Ontario, a strong relationship between supply and utilization but a mismatch between supply and population need. Our results raise fundamental questions about psychiatrists’ scope of practice and how these physicians should be incentivized to meet the population’s mental health needs. The typical response to poor access to physicians is to conclude that more physicians are needed. If the patterns seen in this study persist, increasing psychiatrist supply will have little impact on patients’ access to essential services.
That last point is very strong and worth repeating: increasing psychiatrist supply will have little impact on patients’ access.
It’s not surprising to see that this paper has sparked criticism. For example, at the CPA meeting, the quality of the dataset was questioned. Sure Kurdyak et al. looked at OHIP billings – but, as was argued, many doctors are on alternative funding models. Looking at OHIP billings as a way of considering practice patterns in Ontario, then, is like looking at real estate pricing in downtown Toronto and drawing conclusions for the whole province. It’s a good argument, but Dr. Kurdyak responded by pointing out that the data did consider shadow billing – with no material effect on the findings.
What then to make of the larger point about a supply-population need “mismatch?” Should psychiatric practice focus on more acute management (and, the corollary: less on long-term therapies)? Should compensation and hospital reimbursement reflect this? Are alternative, less-physician focused teams needed? Like any great paper, Kurdyak et al. end up asking more questions then they answer. At its core, the Kurdyak et al. paper suggests that we could be more creative in the organization and compensation of psychiatric care. Based on the CPA discussion, from a provider perspective, this may be unsettling. But from a patient perspective, the data fundamentally supports their point. And, as my tearful patient noticed, the current system falls short for psychiatric patients.
Reading of the Week. Every week I pick a reading — often an article or a paper — from the world of Psychiatry.
Recent Comments