From the Editor
It’s an effective treatment for depression – maybe the most effective. Yet ECT remains highly controversial. Patients routinely ask about its safety; the media portrayal is tough.
This week, we look at two new studies on electroconvulsive therapy. In the first, just published in The Canadian Journal of Psychiatry, the authors consider the use of ECT in Quebec over a 15-year period, finding a decline over time.
 An ECT Machine: going the way of the dodo bird?
An ECT Machine: going the way of the dodo bird?
We also look at a new paper from Acta Psychiatrica Scandinavica considering the safety of ECT, tapping a rich database.
These new papers point to a public health problem: the treatment is incredibly safe (and effective) but used less and less often.
Note: there will be no Reading next week.
DG
ECT and Use
“Electroconvulsive Therapy Practice in the Province of Quebec: Linked Health Administrative Data Study from 1996 to 2013”
Morgane Lemasson, Julie Haesebaert, Louis Rochette, Eric Pelletier, Alain Lesage, Simon Patry
The Canadian Journal of Psychiatry, 25 October 2017 Online First
http://journals.sagepub.com/doi/full/10.1177/0706743717738492

Electroconvulsive therapy (ECT) is an effective and safe medical intervention, designed to induce a convulsion in the brain to treat some of the most resistant forms of specific psychiatric illnesses. First used in 1938, this therapy was frequently administered before the development of psychiatric medications in the 1960s. Since then, its use varies greatly across countries.
To our knowledge, the first assessment of the practice of ECT in the province of Quebec was published in 2002 by the Agence d’évaluation des technologies et des modes d’intervention en santé (Health Technology Assessment Agency of Quebec, or AETMIS), part of the International Network of Agencies for Health Technology Assessment. Analysis of the physician billing data derived from the Régie de l’assurance maladie du Quebec (Quebec’s health insurance board, or RAMQ) showed an increase in ECT treatment from 1988 to 1996 and then a stabilisation until 2001. The AETMIS report did not indicate the number of people who received ECT, or standardised prevalence. The interprovincial comparison was therefore based on the number of hospitalisations associated with ECT from The Canadian Institute for Health Information (CIHI). Great variability was observed based on these data, with prevalence ranging from 15 to 140 hospitalisations per 100,000 inhabitants. A marked heterogeneity in ECT utilisation was reported among the different regions of Quebec and also among the Canadian provinces.
Interestingly, Quebec and Ontario had among the lowest prevalence rates in Canada between 1999 and 2000, with 26 and 37 hospitalisations per 100,000 inhabitants, respectively. This variability seems, in part, due to differences in the accessibility of this therapy. A recent meta-analysis, addressing the international prevalence of ECT since 1973, estimated the use of ECT at 16.9 treated persons per 100,000 inhabitants globally, with a decreased trend over time and a higher ECT utilisation rate in higher-income countries.
There are several limitations of using only data from hospitalisations or only data from physicians’ billings to analyse ECT utilisation rates. The hospitalisation rate does not make it possible to estimate the number of people treated, as the same patient may have been hospitalised and treated by ECT several times in the same year. This rate also does not include outpatient ECT treatments (performed in outpatient clinics), with one study reporting that outpatient ECT rates increased by 18% to 28% between 1988 and 2001. Likewise, estimations based on billing data may underestimate ECT use by not considering ECTs administered by physicians under remuneration by the hour. Linking different health administrative databases, including hospital and physician payment data, could thus lead to a more accurate estimate of ECT use.
As part of a quality improvement process, the main objectives of this study were to assess the profile of ECT use from 1996 to 2013 and propose a model for routinely monitoring ECT in Canada’s provinces. The secondary objectives were to estimate the overall ECT utilisation prevalence, treatment indications, ECT practices, and the regional volumes of ECT by clinic and by psychiatrist.
 Morgane Lemasson
Morgane Lemasson
So begins a paper by Morgane Lemasson et al.
Here’s what they did:
- The authors drew data from the Quebec Integrated Chronic Disease Surveillance System of the Institut National de Santé Publique du Québec (which links several health administrative databases, including physician payment claims) in the years 1996 to 2013.
- Inclusion criteria included all people aged 18 years and older who had public coverage.
- To be considered as having ECT, a person had to receive at least one treatment during that year. Acute ECT treatment meant that there were given more than one treatment in a week; maintenance meant treatments were given more than seven days apart.
- Data analysis considered gender, age groups, acute and maintenance ECT, and the number of psychiatrists administering it. They also considered trends: “Tests for trends were made by fitting negative binomial regression models.”
Here’s what they found:
- “8,149 individuals received at least one ECT between 1 April 1996 and 31 March 2013 in Quebec.” Most of the cases were identified by physician billing claims and hospital records (75%).
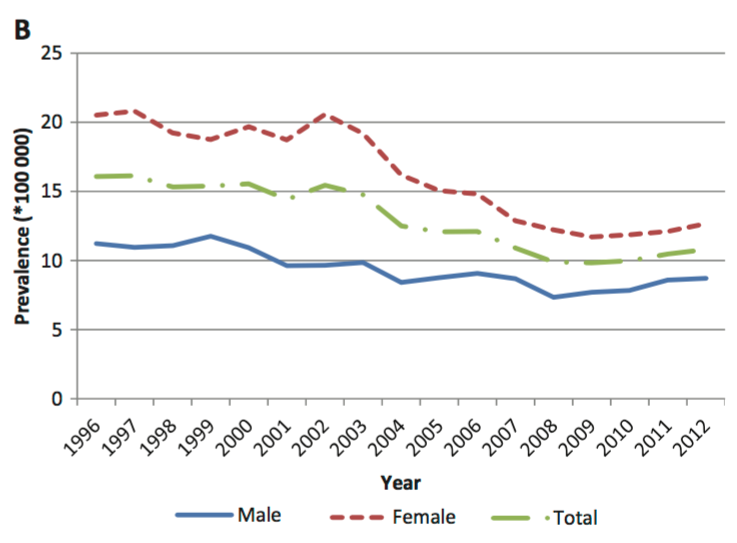
- The trend over 15 years: “with age-standardised rates decreasing from 15 per 100,000 for 1997 to 2002 to 10 per 100,000 for 2008 to 2013.” That’s a decrease of 33%. See the figure below.
- The decrease was observed across all age groups and both genders.
- “The proportion of individuals who exclusively received maintenance treatments increased during the study period, shifting from 5% in 1996 to 16% in 2012. In contrast, the proportion of individuals who exclusively received acute treatments decreased from 72% to 52% over the same period.”
- “The number of psychiatrists who administered ECT varied little during the study period, from 329 psychiatrists in the period of 1998–2001, to 340 in 2003–2006, and 274 in 2008–2012.”
They go on to conclude:
This study provided a detailed picture of ECT use in Quebec from 1996 to 2012 and demonstrated the feasibility of using the QICDSS to identify ECT usage rates. A decrease in the use of ECT has been observed in Quebec for both men and women of all ages. However, regional disparities in ECT use call for a deeper examination of the practice of ECT in Quebec and in Canada.
A few thoughts:
- This is a good paper.
- Though the larger purpose of this study was to look at a way of understanding ECT use, the numbers themselves are interesting. In Quebec, there seems to be a long-term decline in ECT use. And it’s big: a decrease of 33% over the study period.
- Is that generalizable to the country? That’s not clear because so little is really known about ECT treatment. In 2015, a paper examined ECT use nationally based on a survey. Though the approach is reasonable, the response rate wasn’t high.
- Even if ECT prevalence is stable outside Quebec, it’s striking that it would be on decline in the second largest province. So much evidence favours the use of ECT. In a recent Reading, we considered a major paper showing that ECT reduced readmissions after psychiatric hospitalizations. You can find it here: http://davidgratzer.com/reading-of-the-week/reading-of-the-week-ect-and-inpatients-an-underused-tool/.
- But how safe is ECT? One of the criticisms is that it’s actually not that safe. Much work has been done in the area, but a new paper is worth considering. CAMH’s Daniel Blumberger et al. have just published a comprehensive study, “Low medical morbidity and mortality after acute courses of electroconvulsive therapy in a population-based sample.”
You can find it here:
http://onlinelibrary.wiley.com/doi/10.1111/acps.12815/full
In this Acta Psychiatrica Scandinavica paper, they do a population-based cohort study tapping health administrative data from Ontario over the period of 2003 to 2011. They looked at medical events up to a week after ECT, and a month after.
 Daniel Blumberger
Daniel Blumberger
Events were rare, with the most common being falls.
This figure summarizes the results:

{kind=link}
They note:
In a large population-based sample of almost 9000 individuals who were receiving an acute course of ECT between 2003 and 2011, we observed a low rate of severe medical adverse events and an even lower mortality rate of any cause. The most common severe medical adverse events were falls and pneumonia, with the highest risk among older adults, those with a high ASA score, or those with a history of ischemic heart disease. Medical events were rare in individuals under age 65, with less than 1% of individuals in this younger group experiencing one or more adverse events.
They put that in perspective:
Reassuringly, the 7-day mortality rate after ECT in patients 65 years of age and older in our study (0.7 per 10 000 treatments) is still 3–5 times lower than the 7-day mortality after ambulatory surgery in patients 65 years of age and older (2.5–3.5 per 10 000 procedures).
- Safe, effective, and yet declining in use. Ouch.
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments