From the Editor
Well, he looks better.
So often our conversations about patients – in our emergency rooms, wards, and clinics – focus on soft evidence of improvement. No wonder: psychiatry lacks biomarkers. And so, while our colleagues in medicine talk about blood sugars and white blood cell counts, we often discuss other things, like how our patients look and sound.
The promise of measurement-based care: objective evidence of change (or lack thereof). The idea is having a moment, with more and more interest. But what does the literature say?
In the first selection, Maria Zhu (of the University of British Columbia) and her colleagues consider RCTs. In a systematic review and meta-analysis, they look at the efficacy of measurement-based care for depressive disorders. They conclude: “Although benefits for clinical response are unclear, MBC is effective in decreasing depression severity, promoting remission, and improving medication adherence in patients with depressive disorders treated with pharmacotherapy. The results are limited by the small number of included trials, high risk of bias, and significant study heterogeneity.” We discuss the big paper.
The pandemic has changed much with day-to-day practice, including with the rapid virtualization of mental health care. Remember a time when you didn’t need to talk about “being on mute?” And some psychiatrists have been on the front lines of the vaccine effort. In the second selection, Dr. David Goldbloom (of the University of Toronto) writes about his experiences working in a vaccine clinic. His Toronto Lifeessay details the YouTube video he watched to remind himself of how to administer shots, his family ties to vaccinations, and his fondness for the work. “I will always be grateful to have experienced the joy of jabbing.”
DG
Selection 1: “The Efficacy of Measurement-Based Care for Depressive Disorders: Systematic Review and Meta-Analysis of Randomized Controlled Trials”
Maria Zhu, Ran Ha Hong, Tao Yang, et al.
The Journal of Clinical Psychiatry, September/October 2021

Depressive disorders, including major depressive disorder (MDD), are common psychiatric disorders worldwide and a leading contributor to the global burden of disease. Despite many evidence-based pharmacologic and psychosocial interventions, treatment outcomes for depression are relatively poor in clinical practice. A key contributor to poor outcomes may be the unstructured approaches used by clinicians in assessing patient progress that make therapeutic effects difficult to quantify. Clinicians may also have difficulty detecting deterioration of patient symptoms, leading to delay of needed treatment adjustments….
Measurement-based care (MBC) is an evidence-based practice that provides a systematic framework for routine outcome monitoring and has demonstrated benefit in treating a range of psychiatric disorders. MBC includes (1) routine administration of validated rating scales, either by clinician-rated or patient-reported outcomes (PROs); (2) review of scores by practitioners and patients; and (3) using scores to inform shared clinical decision-making. MBC has specifically been recommended for the management of MDD by the American Psychiatric Association (APA), Canadian Network for Mood and Anxiety Treatments (CANMAT), and UK National Institute for Health and Care Excellence (NICE) clinical practice guidelines.
MBC offers several potential benefits for depression management. For example, MBC enables clinicians to individualize depression treatment based on up-to-date information about patient symptoms and severity. Quantifiable patient data can be readily incorporated into medication algorithms, facilitating standardized care. MBC may also help to identify treatment nonresponders, detect residual symptoms, and increase treatment adherence by encouraging patient participation. Although there are recognized barriers and facilitators to implementation and scalability of MBC, its feasibility for depression treatment in clinical settings and propensity to improve patient outcomes were demonstrated in several large trials and projects. Despite these benefits, MBC continues to be underutilized in clinical practice.
So begins a paper by Zhu et al.
Here’s what they did:
- They searched various databases, including MEDLINE (OVID).
- Various search terms were used across four categories: measurement-based care, depressive disorder, antidepressant or psychotherapy, randomized controlled trial.
- “Studies were included if they were (1) RCTs involving (2) adults ≥ 18 years of age (3) currently diagnosed with a depressive disorder based on validated criteria (ie, DSM-IV, DSM-5, or ICD-10) and were given (4) MBC as an intervention.”
- “To be considered MBC, the intervention had to include a routinely administered validated symptom, outcome, or process measure that involved practitioner review of data and use of data to inform clinical decisions.”
- Two independent reviewers extracted the data.
- The primary outcome: clinical response rate (50% or greater improvement from baseline score at end of treatment).
Here’s what they found:
- The initial search found 8,879 articles. After review: “The final 8 articles yielded outcome data from 7 studies for the meta-analysis.”
- Study characteristics. “All the included studies involved pharmacotherapy management… Individual study sample sizes ranged from 108 to 915 participants with a total of 2,019 participants in the 7 studies. The participants in all studies were diagnosed with a depressive disorder or a major depressive episode… Three studies were conducted in outpatient psychiatry settings, 2 studies in outpatient primary care settings, and 2 studies in inpatient psychiatry settings.”
- Meta-analysis with random-effects models found no significant difference between MBC and comparison groups in response rates (3 studies; odds ratio [OR] = 1.66…).
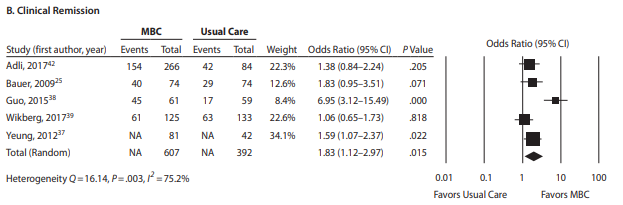
- MBC was associated with significantly greater remission rates (5 studies; OR = 1.83…), lower endpoint severity (5 studies; standardized mean difference = 0.53…), and greater medication adherence (3 studies; OR = 1.68…). See figure below.
A few thoughts:
- This is a good paper.
- A six-word summary: two cheers for measurement-based care. The authors write that “the findings from this systematic review and meta-analysis of RCTs support the use of MBC in the management of depression, particularly with pharmacotherapy.”
- Of course, a systematic review and meta-analysis is only as good as the papers it draws from. The papers look reasonable, and come from different regions of the world, offering different types of practice, including inpatient work. Red flag: bias was an issue. “Two studies were assessed to have an overall low risk of bias, whereas the remaining 5 studies were judged to have a high risk of bias…” Ouch.
- The authors note other limitations, including “the heterogeneity in methodologies of the included studies. Currently, there is no consensus on the most effective measures or the optimal frequency of measurement for MBC.”
- Is measurement-based care more helpful for some types of care? The authors argue it is: “MBC may be particularly relevant to antidepressant prescribing, in which simple algorithms can guide stepwise changes to the dosage or medications depending on measurement outcome. In this regard, favorable outcomes with MBC may in part be due to increased adherence to medication.”
- Measurement-based care has been considered in past Readings, including one that focused on Guo et al. from The American Journal of Psychiatry: https://davidgratzer.com/reading-of-the-week/reading-of-the-week-depression-and-measurement-based-care-depression-week-1-of-3/
The full Journal of Clinical Psychiatry paper can be found here:
https://www.psychiatrist.com/jcp/depression/measurement-based-care-depression/
Selection 2: “‘A teenager left me a thank-you note after her second shot’: This psychiatrist is working as a Covid vaccinator at CAMH”
David Goldbloom
Toronto Life, 28 October 2021
![]()
I work as a psychiatrist at CAMH. In the pre-Covid era, my job mainly consisted of seeing new patients who’d been referred by family physicians and nurse practitioners for diagnostic assessment. People came from all corners of the GTA and beyond, grappling with public transit or parking, forced to take time off work or arrange child care. When the pandemic began, I became, like so many others, a telepsychiatrist, seeing patients all day on a secure video platform from my home into theirs. But something novel brought me back to our hospital site at Queen and Ossington. In April of 2021, I started doing four-hour tours of duty once or twice a week in the CAMH vaccination clinic, sitting at tables in the repurposed gymnasium, a line of eager vaccine recipients snaking the outside the building.
Being a vaccinator reinforces a fundamental sense of my professional and personal identity.
So begins an essay by Dr. Goldbloom.
He notes that he comes from a long line of pediatricians who vaccinated many children. And he mentions his decision to join the vaccination effort: “When the opportunity arose to work in CAMH’s vaccination clinic, I leapt at the chance for me to pitch in beyond my normal clinical work. Selfishly, I was also eager to do something other than sitting at home staring at a monitor. I wanted to interact with patients, families and colleagues.”
He makes various observations:
On the first jab
“As a psychiatrist, it had been a while since I had given an intramuscular injection. After watching a mind-numbing but mandatory one-hour government video on the bureaucratic requirements – followed by an excellent 90-second YouTube video on how to give an intramuscular deltoid injection – I was ready to start. I accompanied a seasoned jabber, my colleague Bernard Le Foll, to an inpatient unit, and after watching him do it twice, I was ready. Frankly, registering patient information on an iPad was more intimidating than sticking the needle in and pushing the plunger.”
On connecting with people
“Psychiatrists traditionally allow an hour to conduct a formal assessment. The vaccine clinic encounters are much briefer – and a powerful reminder of how much we can find out about people in a matter of minutes. I learn what is important to them, what they fear, and what they enjoy. I’ve realized I can do something positive for someone in a short period of time and make the experience as helpful as possible. A young teenager who came back to me for her second injection shyly left me a thank-you note for making the process easier for her – and included a Tim’s gift card. It was a sweet encounter.”
On the joy of jabbing
“First and foremost, after our long period of isolation, it is great to be among colleagues and patients without having to say, ‘You’re on mute,’ or to ask them a question without clicking on a raise-hand icon. Wiping someone’s shoulder clean with an alcohol swab, gently pinching some flesh, inserting the needle, and applying the band-aid are all moments of connection. It’s remarkably different from the rest of my work. How often do 10 to 12 people thank you in a meaningful way every hour? How often do you get to feel that you are making a small but useful contribution to fighting an illness that threatens all of us? And how often do you get to witness at close range such immediate and palpable relief? Recently, two patients wept with happiness on receiving their second dose (one warned me beforehand, ‘I’m going to cry but I’m not upset’).”
A few thoughts:
- What a terrific article.
- There are many great lines in it. This one made me laugh: “I have never seen so many tattoos.”
- Psychiatric work can take many forms: psychoanalysis, bench research, medication management, and more. Add to the list: vaccinations during a once-in-a-century pandemic.
- For those who want to read more by Dr. Goldbloom, the except of his recent book was featured in a past Reading. The link: https://davidgratzer.com/reading-of-the-week/reading-of-the-week-dr-david-goldblooms-new-book-on-innovation-and-mental-health-care/.
The full Toronto Life essay can be found here:
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments