From the Editor
Today is the 75th anniversary of D-Day.
Ceremonies are planned across the country, and across Europe; Prime Minister Justin Trudeau is in France. During these anniversaries, people comment on the importance of the moment. US President Barack Obama noted: “much of the progress that would define the 20th century, on both sides of the Atlantic, came down to the battle for a slice of beach only six miles long and two miles wide.” And people speak of the loss of life. US President Ronald Reagan, on a past anniversary, talked about “the boys of Pointe du Hoc” who had tried to take “these cliffs” off the beaches, noting that the majority were killed.
But the damage of war is not only in the loss of life.
In this week’s Reading, we consider shell shock and PTSD starting with the first paper on the topic, written by Dr. Charles S. Myers for The Lancet, published just over a century ago. Dr. Myers writes about three cases of shell shock, noting the similarities in their presentations.

We also consider a recent paper, published in JAMA Internal Medicine, discussing a more modern presentation – but perhaps not a profoundly different presentation. Finally, we consider a summary of recent published guidelines.
DG
Shell Shock and Observations
“A CONTRIBUTION TO THE STUDY OF SHELL SHOCK: BEING AN ACCOUNT OF THREE CASES OF LOSS OF MEMORY, VISION, SMELL, AND TASTE, ADMITTED INTO THE DUCHESS OF WESTMINSTER’S WAR HOSPITAL, LE TOUQUET”
Charles S. Myers
The Lancet, 13 February 1915
https://jmvh.org/wp-content/uploads/2012/12/A-Contribution-to-the-Study-of-Shellshock.pdf
CASE 1.-Private, aged 20. Admitted on Nov. 5th, 1914. On the nights of Oct. 28th and 29th he slept in Lhe booking hall of X station ; “not much sleep there” On the 30thhe motored in a ’bus from X to Y, arriving there at 7.30 P.M.; billets found at 8 P.M. ; on guard from 10-11.30 P.M., and from 1.45-3.45 A.M. At 11 A.M. on the 31st for the first time he went to the firing line. His platoon advanced to one set of trenches and then crossed the road to another, only to find it filled with cavalry and to be told that there was no room for them. During the retirement from this trench, at 1.30 P.M., they were ‘found’ by the German artillery. Up to that time he had not been feeling afraid; he had ‘rather been enjoying it,’ and was in the best of spirits until the shells burst about him.
He was now retiring over open ground, kneeling on both knees and trying to creep under wire entanglements, when two or three shells burst near him. As he was struggling to disentangle himself from the wire three more shells burst behind and one in front of him. (An eye-witness in this hospital says that his escape was a sheer miracle.) After the shells had burst he succeeded in getting back under the wire entanglements; all his comrades had retired already.
 Charles S. Myers
Charles S. Myers
So begins a paper by Dr. Myers – the first on shell shock.
Dr. Myers reviews the histories. He also considers the distortions in their senses.
To taste and smell, for example, with the first case –
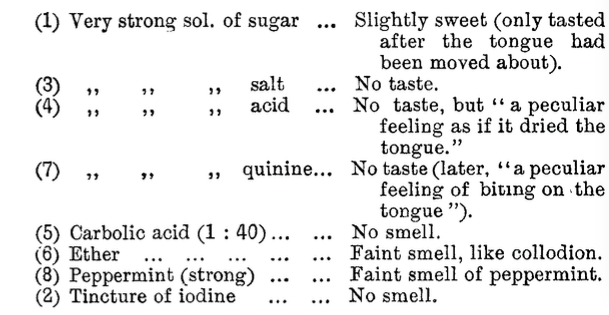
He tries hypnosis. (For the record, case 1 “resisted.”)
He summarizes the findings:
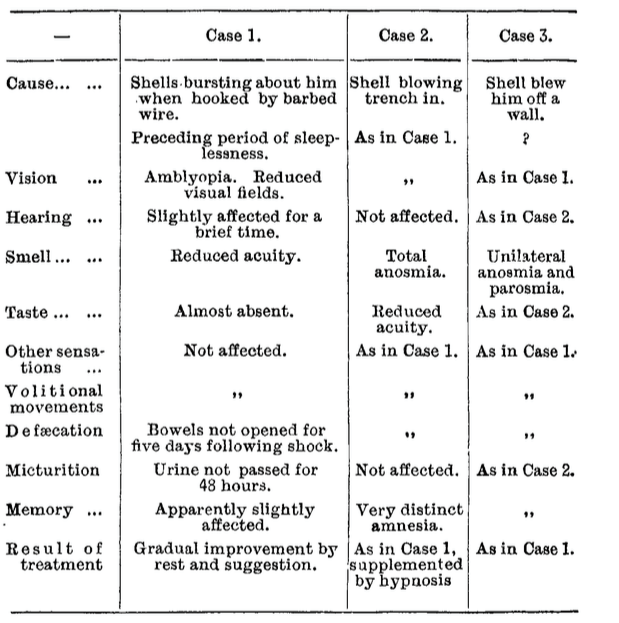
He concludes:
The shells in question appear to have burst with considerable noise, scattering much dust, but this was not attended by the production of odour. It is therefore difficult to understand why hearing should be (practically) unaffected, and the dissociated ‘complex’ be confined to the senses of sight, smell, and taste (and to memory). The close relation of these cases to those of ‘hysteria’ appears fairly certain.
A few thoughts:
- This is a fascinating paper.
- Dr. Myers lacked the tools of modern medicine – none of these three patients had neuro-imaging, for example – but he was a keen observer and made excellent observations.
- Dr. Myers survived the war,but was deeply frustrated. He maintained that shell shock could be a treatable condition – though was unable convince the military leadership.
PTSD and Reflections
“Memorial Day Reflections – The Invisible Enemy”
Kim Chen
JAMA Internal Medicine, November 2018
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2701620
It was a decade ago when I first met Dennis, an unassuming Vietnam veteran seeking treatment for gastroesophageal reflux disease, onychomycosis, and posttraumatic stress disorder (PTSD). It was not until the second visit, though, when I realized how profound his issues were. While reaching across the triangular-shaped room to get a blood pressure cuff, I accidently kicked a rolling stool. In a split second, Dennis, who had been resting easily in his chair, was sprawled on the floor on his hands and knees, tense and hyperalert. I apologized profusely for alarming him, and after a few deep breaths he responded, ‘It’s ok. I do this all the time. I can’t help it.’
So begins a short paper by Dr. Chen.
The paper describes the deep problems the illness has had on the patient’s life. “His boss explained to the clients, ‘It’s just his P-T-S-D. You know, shell shock.’” Though initially understanding, his employer lets him go.
While many medications are tried, the patient doesn’t do particularly well.
In the 10 years that I have known Dennis, we have made no progress on his startle response. We have tried a multitude of medications, cognitive therapies, eye movement desensitization and reprocessing, prolonged exposure therapy, battlefield acupuncture, and marijuana. Each new treatment or subspecialty referral brings the prospect of a normal life but ends in futility.
A few thoughts:
- This is a moving piece.
- A century has passed since Dr. Myers wrote his three cases, and much has changed. For people like Dennis, however, too little has changed.
- What are evidence-based treatments? The next paper summarizes the latest guidelines.
PTSD and Management
“Management of Posttraumatic Stress Disorder”
Michael J. Ostacher and Adam S. Cifu
JAMA, 15 January 2019
https://jamanetwork.com/journals/jama/fullarticle/2719367?resultClick=1
Individuals who have been personally or indirectly exposed to actual or threatened death, serious injury, or sexual violence have a wide range of psychological responses, from transient, nondebilitating reactions to symptoms that meet the Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition) criteria for acute stress disorder or PTSD. Between 6% and 7% of adults in the US general population are estimated to experience PTSD during their lifetime. The prevalence is higher in women than in men. In 2016, 10.6% of veterans receiving care in the Veterans Health Administration had a diagnosis of PTSD. Among veterans who served in Iraq and/or Afghanistan, 26.7% of those seeking care in the Veterans Health Administration receive a PTSD diagnosis.
 Michael J. Ostacher
Michael J. Ostacher
So begins the summary of the 2017 clinical practice guidance from the US Department of Veterans Affairs/US Department of Defense on management of posttraumatic stress disorder and acute stress disorder; Drs. Ostacher and Cifu are concise.
The paper reviews the major recommendations:
- “Individual, manualized trauma-focused psychotherapy (TFP) that has a primary component of exposure and/or cognitive restructuring is recommended over pharmacologic and other nonpharmacologic interventions for primary treatment of PTSD (strong recommendation; quality of evidence not stated).”
- “When individual TFP is not readily available or not preferred by a patient, pharmacotherapy with sertraline, paroxetine, fluoxetine, or venlafaxine (weak recommendation; moderate-quality evidence) or individual non–trauma-based psychotherapy (weak recommendation; quality of evidence not stated) is recommended. There is insufficient evidence to recommend pharmacotherapy over non–trauma-based psychotherapy.”
- “The guideline recommends against prazosin as monotherapy or adjunctive pharmacotherapy for PTSD (weak recommendation; moderate-quality evidence) and makes no recommendation for or against prazosin for PTSD-related nightmares (moderate-quality evidence).”
The authors discuss the recommendations.
The primary recommendation for use of individual, manualized TFP—which includes cognitive processing therapy and prolonged exposure therapy—is based on comparisons of effect sizes in meta-analyses and on studies in which the effect may be exaggerated because of methodology (the effect size of psychotherapy is often greater when compared with wait-list controls rather than with active treatment).
The guideline’s recommendation against use of prazosin is in contrast to its widespread use in current management of PTSD.
In terms of conflicts of interest: “The issue of potential conflict of interest of a guideline written by the DoD and the VA is important to acknowledge. The DoD has an interest in keeping fighting forces at the ready and the VA must adhere to a global budget for delivering care.”
A few thoughts:
- This is a good summary.
- They seem to hesitate on the prazosin recommendation. Though often used, there is little evidence to support this medication, as shown by a major NEJM paper. (Considered in a past Reading, see: http://davidgratzer.com/reading-of-the-week/reading-of-the-week-prazosin-for-ptsd-nightmares-no-better-than-placebo-the-new-nejm-paper/.)
- The most important recommendation is therapy – though that is probably inaccessible to many patients.
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments