From the Editor
It’s like the script of a movie: a doctor seeks a treatment for the nightmares so common in vets with PTSD. He finds an old blood pressure medication that seems to work. Then, after years of use and with some money from a not-for-profit, he does the definitive study, landing a big paper in one of the biggest psychiatric journals.
Dr. Murray Raskind had explained his interest in prazosin simply – he theorized that if he calms the brains of veterans, they would have fewer nightmares. To that end, he sought a medication that would block norepinephrine and found just one antihypertensive that did that, and crossed the blood-brain barrier. And so began a 20-year interest in an old antihypertensive.
But is there a twist in the plot? A new study just published in The New England Journal of Medicine suggests yes. “This 26-week trial involving military veterans with chronic PTSD failed to show a benefit of prazosin over placebo in reducing the frequency and intensity of trauma-related nightmares.”
And, by the way, the lead author of this study is Murray Raskind.
 New pill, same old problem?
New pill, same old problem?
In this week’s Reading, we consider the Raskind et al. study. We also consider the accompanying Editorial that calls the results: “surprising and disappointing.”
DG
Prazosin and PTSD
“Trial of Prazosin for Post-Traumatic Stress Disorder in Military Veterans”
Murray A. Raskind, Elaine R. Peskind, Bruce Chow, Crystal Harris, Anne Davis-Karim, et al.
The New England Journal of Medicine, 8 February 2018
http://www.nejm.org/doi/full/10.1056/NEJMoa1507598?query=featured_home
Trauma-related nightmares and sleep disturbance are common symptoms of post-traumatic stress disorder (PTSD). Enhanced central nervous system adrenergic activity and its persistence during sleep provide a rationale for the use of antiadrenergic medications to ameliorate these symptoms. Animal models support antagonism of the postsynaptic α1-adrenergic receptor of the central nervous system as a target for PTSD treatment. Of the clinically available α1-adrenergic antagonists, prazosin most readily enters the central nervous system.
Six randomized, placebo-controlled clinical trials, in which the number of participants ranged from 10 to 100, showed moderate to large effects of prazosin in alleviating chronic nighttime PTSD symptoms and in improving overall clinical status. Four trials involved U.S. military veterans or active-duty service members, one involved U.S. civilians, and one involved both Iranian military veterans and Iranian civilians. Three trials showed benefits with respect to trauma-related nightmares, change in overall clinical status, and total PTSD symptoms; two showed benefits with respect to trauma-related nightmares, sleep quality, and change in overall clinical status; and one showed benefits with respect to sleep quality and daytime PTSD symptoms. These effects of the drug were observed in some, but not in other, measures of sleep quality and PTSD symptoms. However, the duration of these positive trials was shorter than 15 weeks, and the trials were of moderate size. There are limited data on the ability of prazosin to have sustained efficacy for chronic PTSD symptoms over longer periods. We conducted the Prazosin and Combat Trauma PTSD (PACT) trial to determine the efficacy of prazosin in patients with chronic combat-related PTSD who had frequent nightmares. We hypothesized that veterans randomly assigned to prazosin would have less frequent and less intense trauma-related nightmares, greater improvement in sleep quality, and greater improvement in overall clinical status (the three primary outcome measures) than veterans assigned to placebo after short-term treatment (10 weeks) and improvement in at least one of the three primary outcome measures after longer-term treatment (26 weeks).
 Murray A. Raskind
Murray A. Raskind
So begins a new paper by Raskind et al.
Here’s what they did:
- “The PACT trial was a 26-week, multicenter, double-blind, randomized, controlled trial that was conducted at 13 Veterans Affairs (VA) medical centers.”
- Inclusion criteria included a diagnosis of PTSD (as determined by DSM-IV and a total score of at least 50 on the 17-item Clinician-Administered PTSD Scale, or CAPS) and reported frequent nightmares.
- Exclusion criteria included acute or unstable medical illness; low blood pressure; the use of cocaine or stimulants.
- Participants were randomly assigned to two groups: those receiving prazosin and those receiving placebo for 26 weeks. Both the drug and the placebo were administered in increasing doses over the course of 5 weeks (prazosin to a daily maximum of 20 mg in men and 12 mg in women). After week 10, participants continued to receive prazosin or placebo in a double-blind fashion for an additional 16 weeks.
- The outcome measures included a change in terms of nightmares (as measured by item B2 on the CAPS), a change in terms of sleep quality (as measured by the Pittsburgh Sleep Quality Index, or PSQI) and overall change (as measured by the Clinical Global Impression of Change, or CGIC).
- Statistical analyses were done.
Here’s what they found:
- “Participants were recruited during the period from January 2010 through August 2012…”
- “The two groups did not differ significantly at baseline with respect to age; race; the experience of war-zone trauma before versus on or after October 7, 2001; behavioral ratings; coexisting psychiatric disorders; or disability status.”
- “Of the 413 persons who were screened at the 12 trial sites, 304 (74%) underwent randomization, and 152 were assigned to each group. A total of 271 participants (90% in the prazosin group and 89% in the placebo group) completed the 10-week primary outcome assessments, and 284 (94% in the prazosin group and 93% in the placebo group) completed one or more of the 10-week primary outcome assessments; 59 participants (20% in the prazosin group and 19% in the placebo group) withdrew from the trial before the 26-week visit.”
- “No significant differences between the prazosin group and the placebo group were found for the change from baseline in secondary outcomes at 10 weeks or at 26 weeks… Over the entire 26 weeks, the least-squares mean (±SE) change in total CAPS score was −12.0±1.4 in the prazosin group versus −13.5±1.4 in the placebo group (P=0.48)…” See figures below for a summary of outcomes.
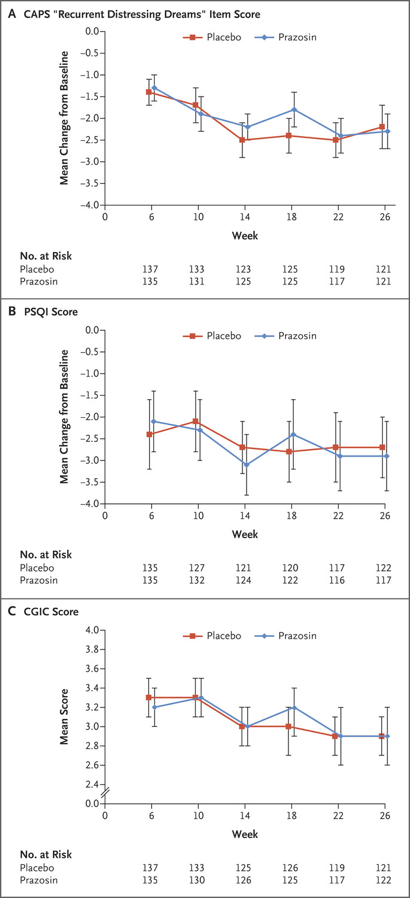
This 26-week trial involving military veterans with chronic PTSD failed to show a benefit of prazosin over placebo in reducing the frequency and intensity of trauma-related nightmares. These results contrast with previous smaller randomized trials of prazosin involving a total of 283 active-duty service members, veterans, and civilian participants, which showed efficacy of prazosin with respect to PTSD-related nightmares, sleep disturbance, and overall clinical function. The failure of the current trial to show benefits does not appear to be attributable to the dose of prazosin, which was higher than in all but one of the previous trials.
Further thoughts:
- This is a good study.
- The result is pretty clear.
- Are there limitations to the study? As the authors note, the patients were “stable.” They write: “The clinical characteristics of patients recruited in this trial suggest that participants had clinically stable PTSD. For example, the lower-than-expected baseline mean blood-pressure levels in this cohort of veterans (among whom the average age was approximately 50 years and who reported high levels of PTSD symptoms) suggest low baseline adrenergic activity, which makes unstable PTSD unlikely.” Did this then colour the results?
- So should prazosin be prescribed to those with PTSD? In an interview, Dr. Raskind said the following: “I don’t think it should change clinical practice — there are six positive studies and one negative study.” It’s a surprising comment given that the results of this NEJM paper – and all the more surprising given that he is the lead author. STAT, an online publication, reports that the VA and Department of Defense, who had access to early results, wrote last year that there was “insufficient evidence to recommend for or against the use of prazosin as … therapy for nightmares or sleep disturbances associated with PTSD.”
- The paper runs with an Editorial by Harvard University’s Kerry J. Ressler. “Alpha-Adrenergic Receptors in PTSD — Failure or Time for Precision Medicine?” is a thoughtful piece, and opens simply and forcefully: “Post-traumatic stress disorder (PTSD) is a debilitating, common, and sometimes deadly psychiatric condition that occurs in the aftermath of extremely distressing and life-threatening exposure to trauma.” You can find the Editorial here: http://www.nejm.org/doi/full/10.1056/NEJMe1716724.
 Kerry J. Ressler
Kerry J. Ressler
He goes on to argue:
Perhaps the most important lesson from this trial is a reminder that PTSD is a cluster of disorders that share trauma exposure as a cause but that can manifest with different combinations of symptoms. Even though rational neuronal system–based therapy, including α1-adrenergic antagonism, may fit neatly with our current understanding of the disorder, only a subgroup of the millions of patients with PTSD may respond to an approach targeting α1-adrenergic receptors. Without recognized biomarkers and intermediate phenotypes that identify patients with dysregulated adrenergic activation, it may not be broadly effective to target this system — particularly in trials that recruit from a population that may already be receiving similar classes of medication.
- So where does that leave us? A major NEJM paper questions the effectiveness of prazosin, but the study is questioned by its lead author. Perhaps we can draw a simple conclusion: prazosin may or may not be helpful for those with PTSD and nightmares, but CBT almost surely is.
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments