From the Editor
Once—and I have never shared this before—I stepped into the street on my walk home from the library. I knew that the bus hurtling through the night would not have time to stop before colliding with my darkly dressed frame, fracturing my bones and scattering my belongings. I imagined my head hitting the asphalt and my brain banging around inside of my skull, bruising irreparably with each impact. I imagined the bus driver’s horror as he turned off the ignition with shaking hands and leapt out of the vehicle to locate my body. It would be a catastrophe that the trauma surgeons could not salvage. I would die.
Rahael Gupta is many things. She’s a graduate of Stanford University, and also Columbia. She’s a medical student. She’s a self-described optimistic. She’s a marathon runner.
And she’s a person who has struggled with depression.

In this week’s Reading, we consider her essay in JAMA. It’s moving and clever and important.
DG
Depression and Recovery
“I Solemnly Share”
Rahael Gupta
JAMA, 13 February 2018
https://jamanetwork.com/journals/jama/fullarticle/2672635
When I was a little girl, my mom or dad would tuck me in at night. I would make each parent complete the ritual of saying goodnight to my stuffed animals and dolls. There was a giant stuffed bunny whose name now escapes me and a multitude of Beanie Babies. There was my Raggedy Ann doll, and there were two plump handmade dolls named Peppermint and Tom. To me, it was essential that each of these entities be kissed and greeted every night, as a reminder that he or she was loved. I was certain the toys would feel terribly sad if neglected. Looking back, I’m sure my parents found this repetitive behavior tiresome, but they tolerated it out of love. This was the first time I remember feeling responsible for the well-being of someone else. “Goodnight, Peppermint,” we would say together. “Goodnight, Tom. Goodnight, Raggedy Ann.”
Twenty years later, I was well into my second year of medical school. I had weathered the storm of the first year of basic sciences and was now struggling to understand neuropathology. I had scored very poorly on the first week’s quiz, so I needed a much higher mark on the second quiz if I wanted to pass the neuroscience sequence.
The night before the second quiz, I remember scrolling through what seemed like an endless series of lecture slides on movement disorders. Each slide presented testable information on the signs, symptoms, genetics, and pathology of different diseases. Like almost everything else in medical school, digesting and memorizing this mass of information felt like an impossible task. Historically, I had outperformed my own expectations, managing a passing grade on each weekly quiz. There was evidence to suggest that I could do this, and yet viscerally, I knew that I could not—not this time.
Something happened within me in the previous months, though I lacked the language to describe it. The chronic anxiety and sleeplessness of the previous year and a half had begun to wear on me.
 The author’s Twitter picture
The author’s Twitter picture
So begins an essay by Gupta.
The piece is very eloquent and doesn’t require much of a summary.
She makes a few points that are worth highlighting:
On Recovery
I realized after that moment that I needed to ask for help. After almost a year of medications and therapy and taking time off school, I am grateful to feel like a stronger, more grounded version of myself. For the first six months of treatment, I stayed extremely private about the state of my health, confiding only in my family and a few very close friends. Yet as time went on, other people approached me with their problems. I willed myself to be more open about my own struggles. It is amazing what you learn when you open up to your fellow medical students. Depression and its vestiges are everywhere.
On Stigmatization (and Physician Health)
We contribute to the stigmatization of mental illness, furthering the notion that dealing with depression is something to be ashamed of, something that should be kept quiet. A recent study estimates the costs associated with physician turnover, decreased productivity, and decreased patient satisfaction due to self-reported symptoms consistent with burnout, noting that system-level change addressing the drivers of burnout, including institutional culture, is both ethically and financially responsible, with an enormous measurable return on investment.
On Depression
Depression is not weakness, though depression is a disease that may make you feel weak. Depression is neither laziness, nor apathy, nor a lack of professional fortitude. It is an expression of an underlying neurobiological pathology about which researchers still have many questions. It is a pathology that, like a many-tentacled octopus, grasps at our emotional stability, our cognition, our sleep, our patience with people, and our will to go on. Depression can obscure our personhood, so that it is hard for others—and for ourselves—to see us for who we really are. Admitting to depression is not weakness but rather is further confirmation of an insidious, life-threatening epidemic in the medical profession. On a very simple level, it constitutes an admission of humanness.
A few thoughts:
- This is a great essay.
- How common is depression in medical students? In 2016, JAMA published a paper on this subject drawing on nearly 200 studies. Rotenstein et al. noted: “This systematic review and meta-analysis of 195 studies involving 129,123 medical students in 47 countries demonstrated that 27.2% (range, 9.3%-55.9%) of students screened positive for depression and that 11.1% (range, 7.4%-24.2%) reported suicidal ideation during medical school. Only 15.7% of students who screened positive for depression reportedly sought treatment. These findings are concerning given that the development of depression and suicidality has been linked to an increased short-term risk of suicide as well as a higher long-term risk of future depressive episodes and morbidity.” You can find the paper here: https://jamanetwork.com/journals/jama/fullarticle/2589340. Another JAMA paper considered depression in residents. You can find the Mata et al. paper here: https://jama.jamanetwork.com/article.aspx?articleid=2474424. And the Reading on this paper can be found here: http://davidgratzer.com/uncategorized/reading-of-the-week-physician-heal-thyself-residents-and-depression-and-more/.
- The papers have a similar methodology (not surprisingly, the corresponding author of the former paper is the first author of the latter paper), and consider depression and depressive symptoms, which partly explains the broad range. Going back to the Rotenstein et al. paper, the authors reported a “crude summary” prevalence of 27.2% drawing on 182 studies. But these studies used different scales and measures. Rotenstein et al. did more analysis: “To further characterize the range of depression or depressive symptom prevalence estimates identified by these methodologically diverse studies, meta-analyses stratified by screening instrument and cutoff score were conducted…” The following figure summarizes their finding:
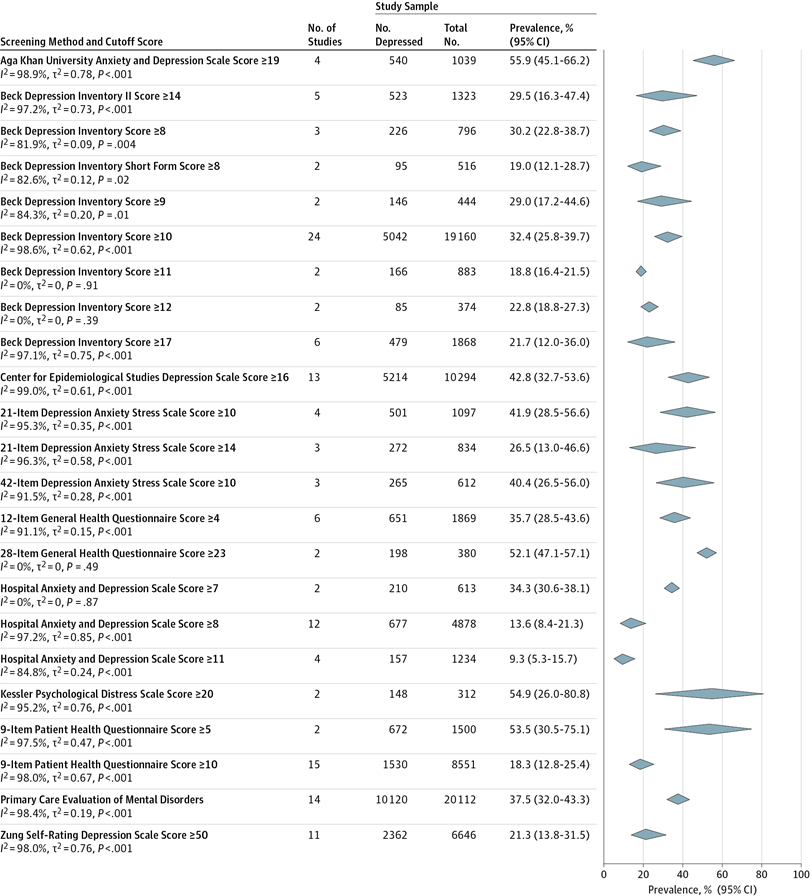 Note the very broad range as represented by blue quadrangles. The point: Rotenstein et al. have done well to draw attention to this issue, but they used many papers across different countries and with different methodologies. Their findings need to be considered in that light.
Note the very broad range as represented by blue quadrangles. The point: Rotenstein et al. have done well to draw attention to this issue, but they used many papers across different countries and with different methodologies. Their findings need to be considered in that light.
- I’m going to repeat the comments made by CAMH’s Dr. David Goldbloom on the Mata et al. paper – “it is a sobering reminder that the white coat is not Kevlar against the illnesses we treat, and our professional culture still has a long way to go in recognizing, accepting and supporting that we get sick, too.”
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments