From the Editor
More physicians are turning to AI scribes to free up time. But what is the impact on clinical care?
In a new JAMA Psychiatry paper, Victor M. Castro (of Harvard University) and his co-authors attempt to answer that question by looking at scribes in primary care. In a cohort study drawing on more than 20 000 routine annual visits, they compared documentation and management of neuropsychiatric symptoms. “Incorporation of AI ambient scribes in primary care was associated with greater levels of neuropsychiatric symptom documentation but lesser likelihood of documented management of psychiatric symptoms.” We consider the paper and its implications.

In the second selection, a letter published in The Canadian Journal of Psychiatry, Dionzie Ong (of the University of British Columbia) and her co-authors consider antidepressant prescribing and evidence, focusing on citalopram and escitalopram. “Preferential prescribing of escitalopram and claims of superiority are not supported by science.”
Finally, in the third selection, Washington Post reporter Dana Hedgpeth writes about the life and death of Carol Sauer, who spent years experiencing homelessness. She had graduated from high school, attended university, and held jobs until 2000, when she became ill. A person who read her death notice on social media comments: “I cried thinking about her. This beautiful woman sitting for 20 years at a bus stop and nobody could make a difference… It’s a reminder of the power and responsibility we have to help those who are homeless and mentally ill.”
DG
Selection 1: “Psychiatric Documentation and Management in Primary Care With Artificial Intelligence Scribe Use”
Victor M. Castro, Thomas H. McCoy, Pilar Verhaak, et al.
JAMA Psychiatry, 21 January 2026 Online First

The use of artificial intelligence (AI) ambient scribes, applying speech recognition and large language models to automate narrative note generation, has rapidly become widespread in medicine. To date, investigations of the impact of this transition to AI scribes are limited. One study suggested that clinicians using ambient scribes spent, on average, 5 minutes less per visit using the electronic health record; others yielded mixed results, with one study suggesting little change in measures of clinician productivity…
In particular, little is known about how the use of ambient scribes may change documentation and management of neuropsychiatric symptoms. Despite efforts to encourage more systematic symptom measurement for depression, prior work suggested that incorporation of the Patient Health Questionnaire-9 (PHQ-9) as a patient-reported outcome was associated with diminished documentation of depressive symptoms. It is possible that use of scribes could ameliorate this diminution, providing clinicians more time to discuss mental health with patients at annual visits and increasing the likelihood that such symptoms are documented. On the other hand, if mental health is not prioritized in the visit, no such shift would be observed.
So begins a paper by Castro et al.
Here’s what they did:
- They conducted a cohort study to “characterize differences in documentation and treatment of psychiatric symptoms in primary care outpatient notes generated using ambient scribes compared with human or no scribes.”
- They used a matched retrospective case-control design to evaluate primary care annual visit notes.
- A random sample of notes from four types of visits – an ambient scribe, a human scribe, without a scribe, and without a scribe prior to scribe deployment – was matched 1:1 using sociodemographic and clinical features.
- Outcome: “Neuropsychiatric symptom documentation, in terms of estimated Research Domain Criteria (RDoC), using a Health Insurance Portability and Accountability Act–compliant large language model (GPT-4o version gpt-4o-11-20; OpenAI); antidepressant prescriptions and diagnostic codes; and referral for mental health follow-up.”
Here’s what they found:
- The analysis included 20 302 notes.
- Demographics & scores. The mean age of the patients was 48 years and 59% of visits were by female patients. The proportion of visits reflecting a PHQ-9 score greater than or equal to 10 (that is, moderate or greater depressive symptoms) was 5.0% overall and was similar across groups.
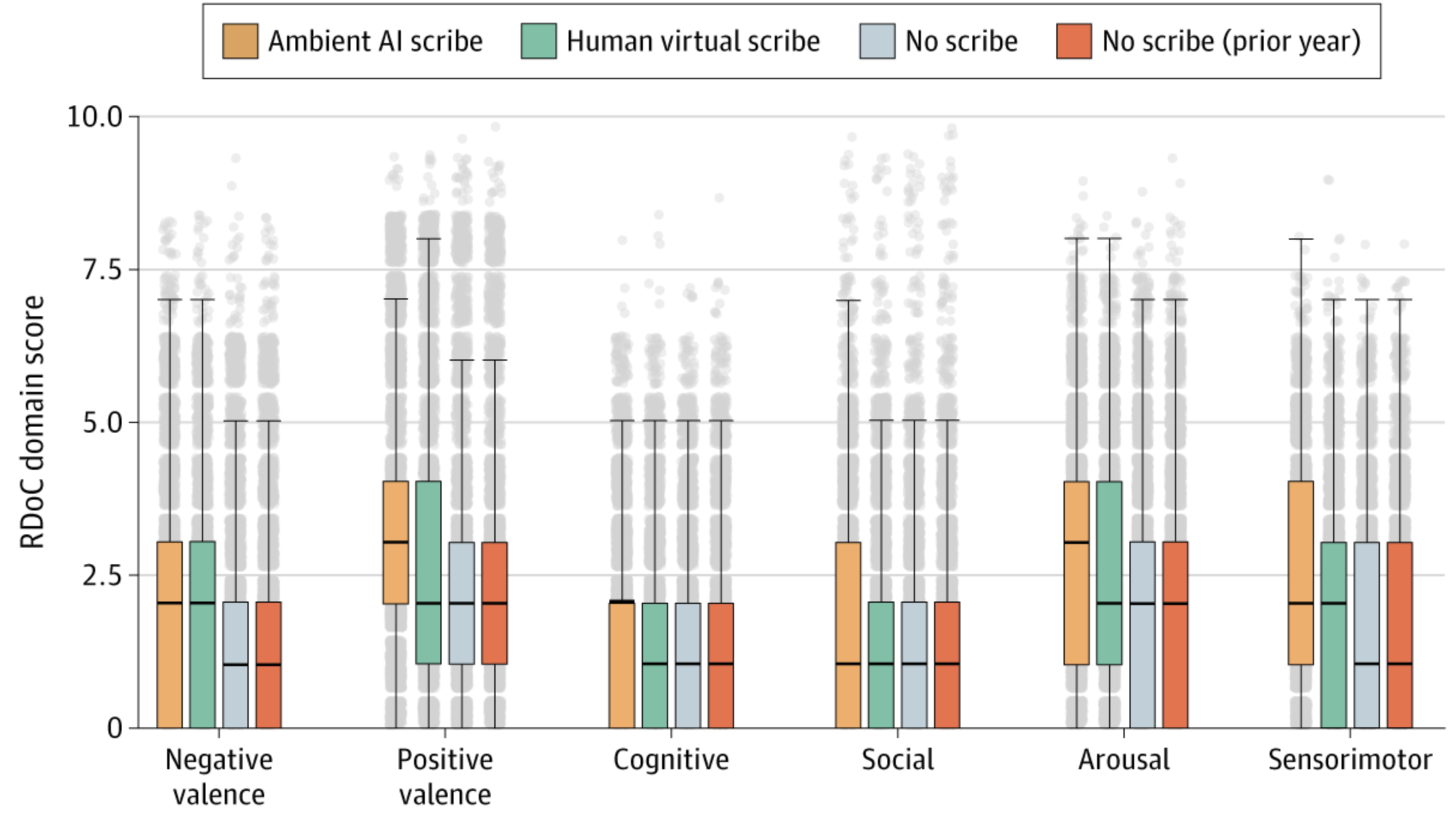
- Neuropsychiatric symptom documentation. “Estimated levels of RDoC symptoms in all 6 domains were significantly greater in the AI-scribed notes compared with other groups.” See figure below.
- Interventions. “In a multiple logistic regression model, likelihood of a psychiatric intervention (referral, new diagnosis, or antidepressant prescription) was significantly lower among AI-scribed visits compared with contemporaneous unscribed visits (adjusted odds ratio, 0.83…), but not for human-scribed visits compared with contemporaneous unscribed visits (adjusted odds ratio, 0.97…).”
A few thoughts:
1. This is a good paper addressing a practical problem and published in a major journal.
2. The main finding in a sentence: “In this study examining clinical documentation from more than 20 000 outpatient annual visits, including roughly 5000 incorporating AI scribes, we found that use of these scribes was associated with greater documented levels of neuropsychiatric symptoms compared with the use of human scribes or no scribe but lesser likelihood of a depression intervention.”
3. This paper makes an important contribution to the literature. Most studies on AI scribes have focused on providers (that is, their workload and satisfaction). But what is the impact on patients? Castro et al. suggest that it may not be neutral.
4. How to understand the main finding? The authors offer: “automating documentation leads clinicians to be less active in general, analogous to reduced proficiency observed in pilots after the emergence of autopilot.” Interesting.
5. Like all studies, there are limitations. The authors note several, including the use of retrospective data. Needless to say, further study is needed.
The full JAMA Psychiatry paper can be found here:
https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2843978
Selection 2: “Rising Escitalopram Use in British Columbia: Is it Rational and Evidence-Informed?”
Dionzie Ong, Simroop Ladhar, Thomas Perry et al.
The Canadian Journal of Psychiatry, 26 December 2025 Online First

Citalopram is a racemic selective serotonin reuptake inhibitor (SSRI) composed of the R(−) enantiomer and S(+) escitalopram, the pharmacologically active S-enantiomer. Escitalopram has been promoted as safer, more efficacious, and faster acting than citalopram for major depressive disorder (MDD). Escitalopram is twice as expensive in Canada, raising the question of whether preferential prescribing is justified. Our objectives were to examine patterns of escitalopram and citalopram use in British Columbia (BC), and to determine whether claims favouring escitalopram are based on science.
So begins a letter by Ong et al.
Here’s what they did:
“We looked at prescription records for the nine most common antidepressants in BC between 2005 and 2024. We also reviewed all the studies that directly compared citalopram with escitalopram. We focused on whether any differences were large enough to matter to patients, whether study results were reliable, and whether studies had problems such as bias or conflicts of interest.”
Here’s what they found:
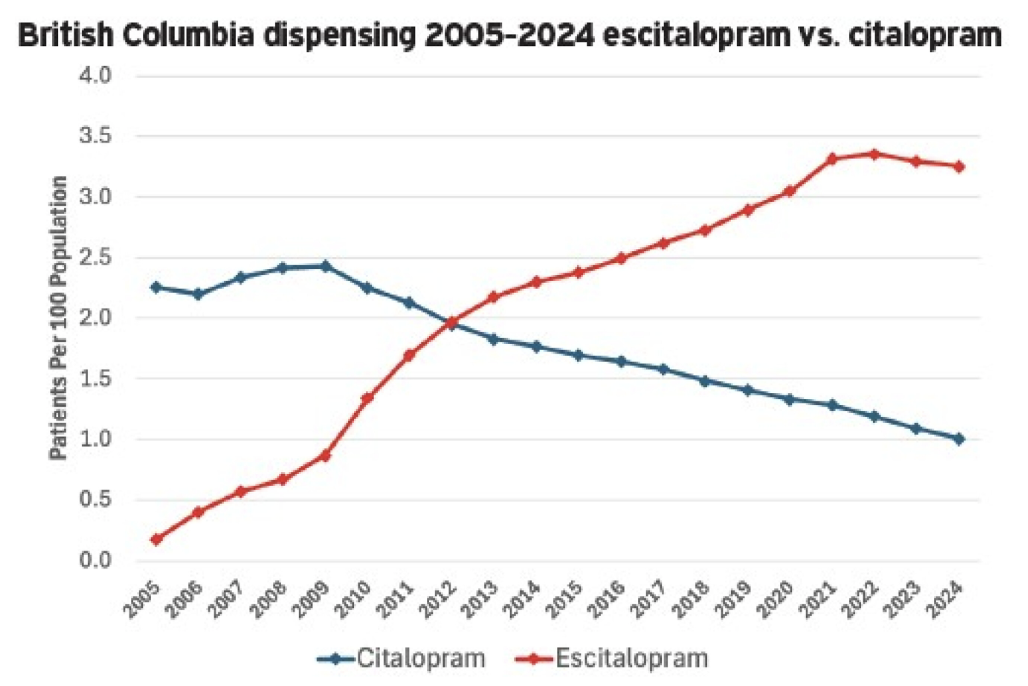
- Prescribing. “Escitalopram use increased after 2009, surpassing citalopram by 2013. It remained BC’s most prescribed antidepressant through 2022 (32 per 1,000 persons/year). Over the same period, citalopram use declined to 12 per 1,000 persons/year.” See figure below.
- RCTs and efficacy. “Four prior reviews cite 12 RCTs comparing escitalopram with citalopram. We identified an additional 4 RCTs for a total of 16. One large multinational RCT was published twice, and 1 of 2 US RCTs (SCT-MD-02) was not published… No RCT reported an efficacy difference exceeding a clinically important threshold.”
- Adverse drug reactions. They were comparable “with no evidence that the R-enantiomer of citalopram worsens safety outcomes.”
A few thoughts:
1. This is a good letter with important data.
2. The main finding in two sentences: “By 2013, escitalopram had become the most prescribed antidepressant in BC, while citalopram use dropped. We found 16 studies that compared the two drugs… None of the studies showed meaningful differences in effectiveness.”
3. How to explain the gap between science and practice? How to address this in the future? Is this a problem of education – or of poor regulation of pharmaceutical industry advertising and promotion?
The full Canadian Journal of Psychiatry letter can be found here:
https://jamanetwork.com/journals/jamapsychiatry/article-abstract/2843977
Selection 3: “She lived on the streets. In a powerful death notice, her family explained why.”
Dana Hedgpeth
The Washington Post, 24 January 2026

For more than two decades, Carol Sauer lived on the streets of Northern Virginia.At 5-foot-2, she became a well-recognized fixture at a bus stop in Arlington. She usually dressed in all black and wore her chic, oversize black sunglasses as she sat on a bench next to her duffel bag, a backpack and a tattered umbrella.
But weeks ago, she wasn’t at her bench. She died New Year’s Eve at a local hospital. The community could have been left wondering what happened to her, but her family wrote a wrenchingly honest death notice that explained who she was and how she ended up living on the streets for decades, despite their frustrating and futile efforts to get her housing and help.
‘Living and dying in her own mind,’ reads the first line. It explains that she died at the age of 66 at 11:28 p.m. at Virginia Hospital Center.
So begins an article by Hedgpeth.
The essay notes that she died from pneumonia and that her family believed she had undiagnosed mental illness that began in her 40s. “After a stranger posted the death notice to a Facebook group, it went viral. Thousands of people reposted it and clicked likes for it. Many commented about how they, too, had struggled to help their loved ones get help for mental illnesses and homelessness and found it increasingly hard at a time when government services for those in need are being cut. Others shared how they had seen Carol at the bus stop and wondered about her story.”
Hedgpeth writes about her life. “Carol was the third of four children raised in Springfield, Virginia. Her mother took care of the family, and her father worked as a commercial airline pilot. As a child, Carol liked reading, swimming at the neighborhood pool and playing the piano. Like her grandmother, she was feisty, and the two were close, often vacationing together.” She graduated high school and attended George Mason University. She had an administrative job for Lockheed Martin in Orlando then moved to Maryland where she worked at the Howard Hughes Medical Institute.
Things changed, however. “In 2000, her family said they started to notice her mental state fraying, as she squirreled away possessions and became fearful people were looking for them.” She lost her job, briefly lived with family, and then became homeless. Her brother tried to help. “For years, he would go around Arlington a few times a month to take her blankets, money, food and hand warmers, often finding her at her usual haunts – the bus stop, the Rosslyn Metro stop and the public library on Quincy Street. She had recently allowed him to put an AirTag in her heavy duffel bag to help track her more easily…. He would invite her to come stay at his house and sometimes she would, spending nearly two hours playing Scrabble with him and accurately keeping score. She would get cleaned up and eat with him and his wife, but inevitably, Bob said, ‘she’d pick a fight’ and leave.”
She was clearly ill. “Carol would often tell her family and others who stopped to check on her at the bus stop that she was homeless because she had been evicted from her apartment by the governor, the county and even the U.S. president. She believed that she would get back her home if she won pending litigation.”
Her brother comments: “She’d never admit she had a mental illness. The people who could help her the most – doctors, psychiatrist – those were the ones she was most afraid of.”
Others tried to help. “La Mont Mitchell, a 71-year-old retired administrator from the local school system who lives a few blocks from her bus stop, gradually became her friend over the past six years. He took her extra hand warmers to ward off frostbite that her brother had left with him. The first thing Mitchell said he noticed when he saw Carol at the bus stop was her signature sunglasses. ‘She was such a classy-looking homeless lady…’”
“She never took his offers of money or food, and when he bought her a black ski outfit to keep warm, she wouldn’t take it. Occasionally, she accepted small packets of trail mix he would buy her at Trader Joe’s.”
The article closes with a discussion of her possessions. “After she died, Carol’s brother started going through her bags. Among the mementos he found: a plaque for her years of service at Howard Hughes, the license plate from her beloved blue Toyota pickup truck that had been towed long ago, old Christmas cards she had received from her family, and a photo of one of her brothers and her niece.”
A few thoughts:
1. This is the kind of obituary that we rarely read.
2. How often do we learn the story of a person we may pass at a bus stop or on a street corner?
3. The family writes about her struggles and raises questions about current law. “As a society, we shouldn’t have to accept laws that set a bar so high that it is nearly impossible for a family to intervene on behalf of a severely mentally ill family member. Though the consequences of the law may be unintended, they are cruel for vulnerable people unable to make rational decisions for themselves. Carol did not like being homeless. Her delusions masked the real reasons why she was living on the street.”
4. Readers may agree or disagree with the family’s perspective, but the tragedy is unmistakable.
The full Washington Post article can be found here:
https://www.washingtonpost.com/dc-md-va/2026/01/24/carol-sauer-mental-illness-arlington
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments