From the Editor
Are people with mental illness more likely to contract COVID-19? Are they at greater risk of dying?
With the pandemic in its eighth month, we think we have answers to these questions, but data is lacking. In the first selection, we consider a new paper, just published in World Psychiatry. QuanQiu Wang (of Case Western Reserve) and her co-authors analyzed a nation‐wide database of electronic health records of 61 million American patients, aiming to assess the impact of mental illness. “These findings identify individuals with a recent diagnosis of a mental disorder as being at increased risk for COVID‐19 infection, which is further exacerbated among African Americans and women, and as having a higher frequency of some adverse outcomes of the infection.”

In the second selection, we consider a new podcast discussing digital tools. I talk with Dr. John Torous (of Harvard University). We discuss apps and mental health. And, yes, he has tips on how to pick apps for your patients and their families.
Finally, in the third selection, we look at a new essay by Dr. Jillian Horton (of the University of Manitoba). Should doctors “stay in their lanes?” She argues against the idea, championing a new activism. “So, to my brothers and sisters in medicine: forget about staying in our lane. This is our call to flood the freeways. We cannot stay parked in neutral. There is no more time.”
Please note: there will be no Reading next week.
DG
Selection 1: “Increased risk of COVID‐19 infection and mortality in people with mental disorders: analysis from electronic health records in the United States”
QuanQiu Wang, Rong Xu, Nora D. Volkow
World Psychiatry, 7 October 2020 Online First
![]()
COVID‐19 infection has rapidly escalated into a global pandemic, with more than 33 million cases and one million deaths worldwide as to September 30, 2020. Socioeconomic deprivation, older age, and several medical conditions are associated with increased risk for severe COVID‐19 disease.
Mental disorders are estimated to affect 20‐25% of the adult population (450 million globally, 47 million in US), and their incidence is likely to have increased during the pandemic, due to a variety of factors. Concerns have been expressed that persons with a pre‐existing mental disorder may represent a population with an increased risk for COVID‐19 infection, and in which the outcomes of the infection are worse.
Multiple factors have been described that could increase the risk of persons with mental disorders to get COVID infection, or make the outcomes of the infection worse. These include challenges in appraising health information and complying with preventive behaviors, limitations in access to health care, homelessness or living in settings where the risk for contagion is higher, and the higher prevalence of comorbid medical conditions that are associated with increased risk for COVID‐19 severe illness (such as cardiovascular diseases, cancers, and chronic obstructive pulmonary disease). Despite the recognition of these multiple vulnerability factors, the risk for COVID‐19 infection and its outcomes among patients with mental disorders have not been investigated systematically.
So begins a paper by Wang et al.
Here’s what they did:
- “We conducted a case‐control study using de‐identified population‐level electronic health records data collected by the IBM Watson Health Explorys from 360 hospitals and 317,000 providers across 50 states in the US, representing 20% of US population.”
- “The status of COVID‐19 was based on the concept “coronavirus infection (disorder)…” while that of mental disorder was based on the diagnosis of “mental disorder (disorder)…”
- “We examined the impact of mental disorders on the risk of COVID‐19 infection, adjusted for age, gender, ethnicity, and common medical comorbidities.”
- “We then explored how demographic factors affected COVID‐19 infection risk among patients with mental disorders.”
- They also looked at rates of death and hospitalization.
- Statistical analyses were done.
Here’s what they found:
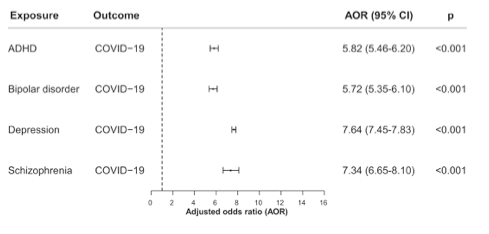
- “Patients with a recent diagnosis of a mental disorder had a significantly increased risk for COVID‐19 infection, an effect strongest for depression (adjusted odds ratio, AOR=7.64…) and schizophrenia (AOR=7.34…).” See figure below.
- “Among patients with a recent diagnosis of a mental disorder, African Americans had higher odds of COVID‐19 infection than Caucasians, with the strongest ethnic disparity for depression (AOR=3.78…).”
- “Women with mental disorders had higher odds of COVID‐19 infection than males, with the strongest gender disparity for ADHD (AOR=2.03…).”
- “Patients with both a recent diagnosis of a mental disorder and COVID‐19 infection had a death rate of 8.5% (vs. 4.7% among COVID‐19 patients with no mental disorder, p<0.001) and a hospitalization rate of 27.4% (vs. 18.6% among COVID‐19 patients with no mental disorder, p<0.001).”
“Based on an analysis of a nation‐wide database of electronic health records in the US, we document that patients with a recent (within past year) diagnosis of a mental disorder have a significantly higher risk for COVID‐19 infection as compared to patients without mental disorders, and also present a worse outcome as evidenced by higher rates of hospitalization and death.”
A few thoughts:
- This is a good and important paper.
- There is much to like here, including the size of the database.
- These findings aren’t surprising (though, of course, they are disappointing). To summarize: our patients are at higher risk of COVID-19, and at much higher risk of dying from the virus.
- The authors note the vulnerability of our patients: “For example, in the case of patients with ADHD, their inattention might place them at higher risk for forgetting to wear face masks or maintaining social distancing, whereas in individuals suffering from depression their amotivation might lead them to neglect protecting themselves or seeking medical attention when indicated, and in a patient with schizophrenia the delusional thinking might lead him/her to reject the use of a face mask.” Issues of equity are at play as well (not surprising, though, of course, disappointing).
- When considering papers on COVID-19, it important to consider the source of the data: in this case, the US. Other studies, including those from countries like South Korea, suggest a different experience. (For the record, the US experience is probably not profoundly different than Canada’s in terms of the pandemic’s effects of those with mental illness.)
- As we consider our response to the pandemic, remembering the most vulnerable among us will be critically important.
The full WP paper can be found here:
https://onlinelibrary.wiley.com/doi/10.1002/wps.20806
Selection 2: “What every physician should know about apps”
John Torous and David Gratzer
Quick Takes Podcast, 18 November 2020

Increasingly, our patients and their families are looking to incorporate apps into their care. What to think? I sat down with one of the leading experts in digital psychiatry, Dr. John Torous of the Harvard-affiliated Beth Israel Deaconess Medical Center, to discuss the potential of apps and their problems.
I highlight from our discussion –
On the popularity of mental health apps, particularly for younger patients:
“Over 50% of our patients have certainly looked at a mental health app, considered it, likely even downloaded to their phones. It’s not the rare patient who tried this…”
On doctors helping patients find apps:
“There are a lot of apps out there, so it can be hard to pick the good ones. But imagine if a patient came to us and said, ‘I’m interested in an antidepressant,’ or ‘I’m interested in therapy.’ And we said, ‘That’s great. Go find one…’”
On app recommendations:
“We’re helping people find a tool that’s going to be useful for them and their mental health. We’re using the same skillset that we have, just for something new.
“The U.S. Veterans Administration, the VA, actually has a ton of really cool, free apps. I recommend: T2 Mood Tracker, to track mood; PTSD Coach, to help people with PTSD; they have several CBT apps that guide you through CBT. Those are all free and really easy to use…”
On chatbots and AI:
“You can imagine talking to a chatbot: the conversation is rather superficial because a lot of mental health is about language and nuance. And, certainly, language can mean different things in different places: if one says something concerning, like, ‘I’m going to walk out this door,’ on an airplane at 30,000 feet that means something different than on the ground level of an office. So chatbots don’t yet understand the context and nuances of language, but I think it’s a rapidly developing area with a lot of excitement.”
On equity:
“We don’t want to make a digital first treatment that the people who need the most help can’t actually partake in.”
 Joining Dr. Torous for a podcast – he’s in the blue shirt
Joining Dr. Torous for a podcast – he’s in the blue shirt
The podcast can be found here, and is just over 19 minutes long:
https://www.porticonetwork.ca/web/podcasts/quick-takes/mental-health-apps
Selection 3: “Forget about our ‘lanes.’ It’s time for doctors to flood the freeways.”
Jillian Horton
Maclean’s, 1 November 2020

The first time somebody told me to stay in my lane, I was 15. I’d gotten a job writing a column about my high school for the local newspaper. The paper’s editor talked to me like I was an actual journalist instead of a kid he’d hired to write about bake sales. Maybe that’s why I quickly evolved to writing about things that felt like they actually mattered.
So begins an essay by Dr. Horton.
On the topic of physicians and advocacy, the Winnipeg internist notes:
In recent months, as more politicians and pundits are telling doctors to stay in their lane, writing has taken on a sense of urgency. And it has also reminded me of an uncomfortable truth about doctors and their lanes: when it comes to public discourse, sometimes we don’t even get on the highway.
She also notes a climate that makes it challenging for physicians to speak out:
But I see an even greater barrier to action for most physicians: Fear. Activism is messy; it attracts criticism or worse. All doctors I know who write or speak in mainstream media have experienced some form of online harassment, and our profession has no existing infrastructure for offering the emotional support and proofing that would amount to better psychological armour. Health officials around the world have been the subject of credible death threats, and harassment takes a cognitive and emotional toll. Anyone who thinks those doctors simply need thicker skin might do well to reflect on what that attitude says about recent tonal shifts in our society.
Yet, she feels advocacy is essential: “So, to my brothers and sisters in medicine: forget about staying in our lane. This is our call to flood the freeways. We cannot stay parked in neutral. There is no more time.”
A few thoughts:
- This is a good essay.
- She makes good points. Physicians, after all, dedicate their lives to helping people. Does the task not involve advocacy? Should the ED physician be silent after seeing the destruction of urban violence and guns? Should the pediatrician not speak out about the problems of corporal punishment?
- But others may challenge this position. To be the devil’s advocate: do we risk undermining our expertise when we comment on things beyond our field? Is there a medical perspective on ecological change – or is that best left to the environmentalists? What about tax policy or government spending?
- Dr. Horton is a skilled writer. Her memoirs will be published in 2021 by Harper Collins. We Are All Perfectly Fine: A Memoir of Love, Medicine and Healing will be in stores in February. I’m excited.
The full Maclean’s essay can be found here:
https://www.macleans.ca/opinion/forget-about-our-lanes-its-time-for-doctors-to-flood-the-freeways/
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments