From the Editor
It’s legal.
After decades of debate, Canada has legalized recreational marijuana, joining an exclusive club of nations with just one other member: Uruguay.
In the coming weeks, many details will be sorted out – some small (the regulation of edibles), some not so small (driving and use). But starting this week, we clinicians work in a different world.
What are the clinical implications of legalization? Will we see more use? How will people present to our EDs and clinics? What should we ask on a history? And how do we treat cannabinoid hyperemesis syndrome? (Spoiler alert: ginger stat.)
In the first selection, I highlight comments by CAMH’s Dr. Jonathan Bertram made in an interview with me. We discuss what every clinician should know about legalization.

And then with an eye on the journals, I pick a few essential articles on cannabis, drawing from The New England Journal, JAMA, and other major publications, considering topics from the adverse effects of marijuana to the implications for pain management.
DG
The Interview
“What All Physicians Need to Know About Cannabis Legalization”
David Gratzer and Jonathan Bertram
Quick Takes, 17 October 2018
I’ve launched a podcast series, hoping to provide us clinicians with relevant and timely information. In our inaugural podcast, released on the day of legalization, I interview Dr. Jonathan Bertram who works in CAMH’s Addiction Division and serves on the board of the Ontario College of Family Physicians.
Our ask?
Just 11 minutes of your time.
You can find the podcast and some additional resources (including resources for patients) here:
https://www.porticonetwork.ca/web/podcasts/quick-takes/cannabis-oct2018
 Jonathan Bertram
Jonathan Bertram
From the interview, I highlight some of Dr. Bertram’s comments.
Think about acute intoxication:
It’s probably someone who’s vitals are not entirely stable, either with really, really high blood pressure, or – in some cases – telling you they feel real faint when they are about to get up (postural hypotension picture); someone who is probably diaphoretic (so sweating quite a bit); and confused by the fact that they are really nauseous and vomiting just because they expected that cannabis was going to do something different… They might tell you that they have just tried cannabis for the first time or they tried something from the store because they wanted to see what it was like or they have been using cannabis for awhile and they decided to go with something they seemed a little like what they normally get… and can’t understand why they are feeling this way.
When taking a history:
The most important thing is getting the typical substance use history – which of course in this case would be a cannabis use history: Identifying if this is the first time they have used cannabis or they have used cannabis before; how long they have been using cannabis for and the means by which they were getting it and the means by which they were using it.
While legalized cannabis is going to be available inhaled, and we are really only looking to see different formulations maybe a year from now, it’s quite possible that they are mixing what they get illicitly with what they were getting from the legalized store – and so the means by which they were getting it is important.
Again, the full podcast is just 11 minutes.
Legalization and the Literature
While it’s true that the literature for cannabis is evolving, there are good and thoughtful papers in this area. With legalization upon us, several recent papers are worth highlighting and considering.
“Adverse Health Effects of Marijuana Use”
Nora D. Volkow, Ruben D. Baler, Wilson M. Compton, Susan R.B. Weiss
The New England Journal of Medicine, 5 June 2014
This paper is a few years old, but the opening seems particularly relevant this week: “In light of the rapidly shifting landscape regarding the legalization of marijuana for medical and recreational purposes, patients may be more likely to ask physicians about its potential adverse and beneficial effects on health. The popular notion seems to be that marijuana is a harmless pleasure, access to which should not be regulated or considered illegal.”
The paper reviews the literature, considering risk of addiction (about 9%), effect on brain development, possible role as gateway drug, relation to mental illness, and risk of motor-vehicle accidents.
This highly readable review does mention conditions that may benefit from cannabis, including MS and AIDS-associated anorexia and wasting syndrome.
I draw attention to the authors’ summary of the increase in potency of marijuana:
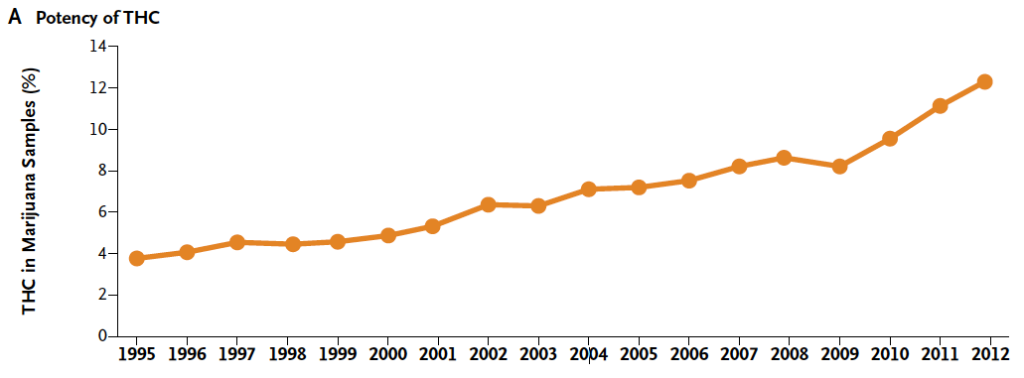
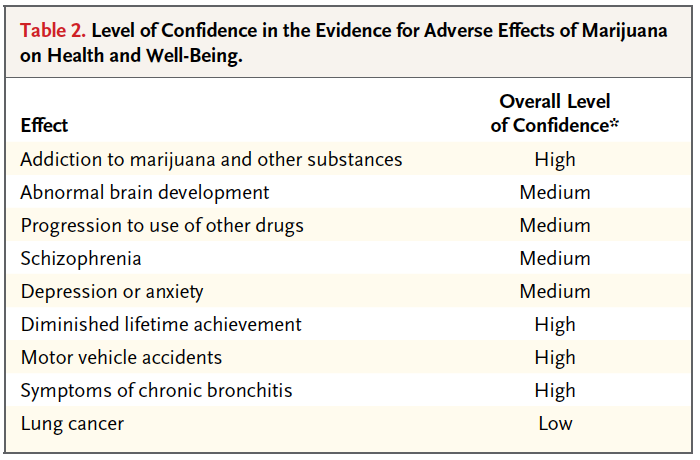
The paper also includes a table on the evidence for adverse effects, with level of confidence.
If you can only read one paper this week, read this one.
https://www.nejm.org/doi/full/10.1056/NEJMra1402309
“Medical Marijuana for Treatment of Chronic Pain and Other Medical and Psychiatric Problems: A Clinical Review”
Kevin P. Hill
JAMA, 23/30 June 2015
This paper uses the case of Mr. Z (a 60 year old man with chronic back pain secondary to a fall decades before) to consider treatment of chronic pain and other conditions with medical marijuana.
Harvard University’s Dr. Hill draws from grand rounds, and is practical yet puts these discussions in a larger policy context (including medical marijuana laws by US state).
With regard to prescribing, Dr. Hill suggests:
The clinical evaluation should start with the patient expressing how they think medical marijuana will be helpful to treat their medical condition. The physician should take a careful history with special focus on previous treatments for the debilitating condition and possible contraindications for medical marijuana such as anxiety disorders, mood disorders, psychotic disorders, and substance use disorders. A thorough risk-benefit discussion should follow, covering both the adverse health effects of marijuana along with the scientific evidence from studies investigating marijuana or cannabinoids as pharmacotherapy for the debilitating condition being treated. It may be useful to provide a context for medical consensus by informing the patient that there currently is little support from major medical organizations for the use of medical marijuana.
The paper includes a nice review of the 28 randomized clinical trials for cannabinoids as pharmacotherapy (beyond cancer treatment), finding: “Use of marijuana for chronic pain, neuropathic pain, and spasticity due to multiple sclerosis is supported by high-quality evidence.”
https://jamanetwork.com/journals/jama/article-abstract/2338266
“US Epidemiology of Cannabis Use and Associated Problems”
Deborah S. Hasin
Neuropsychopharmacology, 30 August 2017 Open Access
“Adults and adolescents increasingly view cannabis as harmless, and some can use cannabis without harm.” So opens Columbia University’s Prof. Hasin does a thoughtful review casting doubt on this view.
The paper is quite exhaustive, covering the effects of prenatal, childhood, adolescent, and adult exposure. The paper is practical for clinicians, and explains cannabis withdrawal symptoms. Where this paper really shines, though, is in drawing in time trends, and showing the evolving picture of marijuana use, legalization, and misuse in the United States.
For the record, in terms of legalization:

https://www.nature.com/articles/npp2017198
“Why it is probably too soon to assess the public health effects of legalisation of recreational cannabis use in the USA”
Wayne Hall, Michael Lynskey
Lancet Psychiatry, 28 June 2016
This paper begins by discussing the legalization of cannabis for recreational use in four US states (Washington and Colorado in 2012; Oregon and Alaska in 2014). The authors consider the effects on public health, given that “[i]n the long run, if more states legalise cannabis, its price is likely to fall well below the black market price…”
But the authors pivot, and consider the American experience with alcohol and tobacco. Here is where this paper shines. They argue that a for-profit cannabis industry will promote the drug, encouraging use and increasing social acceptance. The policy implications are clear, including possible “restrictions on various licensed producers and sellers.”
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(16)30071-2/fulltext
A quick word of thanks to those who made this Reading possible. Thanks to Stephanie Sliekers, Lawrie Korec, Brennan Sarich, Annie Hart, Catherine Laroche Boisvert, Vanessa Alexander, and Caroline Hebblethwaite of CAMH Education for their help in bringing the podcast to life. Thanks to Dr. Peter Selby for explaining cannabis issues to me and Dr. Tony George for his suggestions of relevant papers. And many thanks to Dr. Jonathan Bertram for the interview.
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
October 18, 2018 at 11:56 am
Hi there:
A few points from a practicing emergency physician and cannabis educator.
Acute overdoses mostly present with dizziness and nausea in the emergency department. Vomiting is relatively rare. Diaphoresis is uncommon – can’t say I have ever seen it in a cannabis overdose. The most common complaint is feeling dizzy and fuzzy in the head. People who have overdosed from smoking are generally ambulatory and are more likely to feel anxious. With the higher doses that edibles offer, these are usually more likely to require a stretcher, a blanket, a snack and some time before they are ready to be discharged.
Both inhaled and oral formulations are available at recreational stores – not just inhaled as your expert stated. Oils and gel caps are available. It is edibles that will not be legalized for another year.
Very high blood pressure would be an alarm for another condition as THC is generally associated with lower blood pressure
I would recommend the recent Hill paper over the NEJM Volkow one. This was reviewed by the Poison Review around the time it came out and should really be viewed as much as a political paper as a scientific one.
“I looked at the Volkow article again in preparation for an upcoming podcast, and was struck even more by the bias evident in its discussion. As you note, this is especially apparent in Table 2, “Level of Confidence in the Evidence for Adverse Effects of Marijuana on Health and Well-Being.” Some of the conclusions in that table are not supported by evidence presented, and contradict other sections of the paper.”
She is also recently on record as saying that there has been fentanyl contamination of cannabis. This is a common rumor, even recently spread by the codirector of McMasters Medical cannabis research center, but has zero evidence to support it. This rumor was rebutted by our Health Minister, but unfortunately, irresponsible politicians, police and physicians continue to spread it.
Anyone who is treating cannabis hyperemesis syndrome should be aware of capsaicin more than ginger. Capsaicin is a directed treatment for CHS that likely targets the vanilloid receptors. While ginger may be nice, it does not appear to have any evidence to support its use in CHS and does not appear in the treatment protocol that was recently published by Lapointe, et al.
Yours,
Ian Mitchell