From the Editor
Can a parent’s trauma influence the development of mental illness in his or her child? Research suggests an intergenerational link for several disorders, including PTSD. But what about schizophrenia? Complicating such research: the complexity of genetics, environment, and trauma – and the limits of data.
In a new American Journal of Psychiatry paper, published last week, Iaroslav Youssim (of the Hebrew University of Jerusalem) and his co-authors attempt to answer these questions by looking at parental exposure to the Holocaust – years before conception – and the associated risk of schizophrenia in their children. They drew data from 92 000 births in West Jerusalem between 1964 and 1976. “Offspring of mothers who were older than age 5 when Nazi persecutions began showed over a twofold increase in schizophrenia risk, underscoring the potential impact of trauma and its timing during the preconception period in the pathogenesis of schizophrenia.” We consider the study and its implications.

How often do adolescents and young adults use AI chatbots for mental health? In the second selection, from JAMA Pediatrics, Ryan K. McBain (of RAND) and his co-authors report on a US survey. They find that one in five youth use AI chatbots for mental health advice. “AI chatbots are already embedded in many youths’ mental health information ecosystem, underscoring the need for parents and clinicians to proactively discuss chatbot use to promote safety, appropriate expectations, and linkages to evidence-based care.”
And in the third selection, Sarah M. Gunther discusses medications and her journey in Psychiatric Services. In her personal essay, she describes trying different meds over time and the problems that they caused. She finally lands on the right combination. “I tell this story so that others won’t give up, and so doctors can see that the medications that they prescribe can make an illness worse.”
DG
Selection 1: “Schizophrenia in Offspring of Holocaust Survivors: Intergenerational Effects of Preconception Parental Trauma Within the Jerusalem Perinatal Study”
Iaroslav Youssim, Salomon Israel, Ronit Calderon-Margalit, et al.
The American Journal of Psychiatry, 2 June 2026 Online First

Schizophrenia is a chronic neuropsychiatric disorder typically appearing in late adolescence or early adulthood… Previous research has implicated a number of early-life risk factors in the etiology of schizophrenia, now widely regarded as a neurodevelopmental disorder… With respect to trauma, most human studies have focused on maternal trauma during the pregnancy rather than on the mother’s childhood trauma… To study the impact of objective parental stressors on offspring health in humans, which obviously cannot be done in experimental designs, trauma-based research often focuses on stress-inducing settings of armed conflicts or war-induced adverse conditions. The genocide perpetrated by Nazi Germany against individuals of Jewish ancestry during World War II, known as the Holocaust, reflects an extreme example of a prolonged and multifaceted atrocity, exposing victims to severe stress through persecutions, displacement, starvation, and systematic extermination. Some studies have shown altered mental and physical health in offspring of Holocaust survivors, with higher susceptibility to posttraumatic stress disorder (PTSD), anxiety, depression, substance misuse, lower cortisol levels, and epigenetic changes such as reduced FKBP5 methylation compared to unexposed peers…. In the single study to date that has examined the link between parental Holocaust exposure and schizophrenia in offspring born years later, a difference between exposed and unexposed offspring was found only in schizophrenia rehospitalizations and not in incidence.
These inconsistencies in findings suggest that intergenerational effects of parental trauma likely reflect complex interactions between environmental and personal factors, including features of the preconception traumatic setting and characteristics of both parents and children. Of relevance here is the historical trauma paradigm, which refers to psychological and emotional wounding experienced by a group of people as a result of shared traumatic events such as slavery, colonialism, and genocide. This paradigm extends the intergenerational trauma framework, which traditionally focused on family-level processes, by viewing historical trauma as a collective phenomenon operating at the individual, community, and societal levels.
So begins a paper by Youssim et al.
Here’s what they did:
- The authors used a large, population-based birth cohort (the Jerusalem Perinatal Study) and linked it to Israel’s National Psychiatric Registry to identify offspring who later developed schizophrenia.
- They classified exposure as “parents from European countries under Nazi rule who immigrated to Israel after the anti-Jewish persecutions began.” They focused on age: “Parents were further categorized by their own age (≤5 or >5 years) when the persecutions began.” (!) “Unexposed parents were of European descent not living under Nazi rule.”
- They followed offspring into adulthood and compared the risk of schizophrenia hospitalization across exposure groups.
- Different statistical analyses were done, with maternal and paternal exposures studied separately, and including the use of Cox models to analyze time to first schizophrenia hospitalization.
Here’s what they found:
- There were two subsamples: 14 759 offspring of 7 316 mothers and 18 085 offspring of 8 833 fathers, of whom 3 913 had exposed mothers and 5 672 had exposed fathers.
- Exposure under five years. No associations were observed in offspring whose parents were exposed early.
- Exposure older than five years. Offspring of parents who were older than age five at exposure showed elevated schizophrenia rates (maternal exposure: hazard ratio=2.71; paternal exposure: hazard ratio=1.52).
- Sociodemographic variables. Adjustments diminished the association of paternal exposure at age after five, whereas association with maternal exposure remained strong (hazard ratio=2.38) and withstood further adjustments for covariates.
A few thoughts:
1. This is a bold study, drawing on impressive data with practical questions, published in a major journal.
2. The main findings in two sentences: “children born at least two decades after World War II to women who were over 5 years old when the Nazi persecutions began in their countries faced over a twofold increase in risk of schizophrenia compared to offspring of unexposed mothers. This association was independent of the robust effect of maternal psychiatric hospitalization history and other potential confounders on offspring schizophrenia.”
3. Interesting.
4. Why would exposure age be important? The authors note that “the perception of environmental danger may depend on cognitive development, as children’s risk perceptions evolve with their cognitive, social, and psychological maturation.”
5. Interesting – but is it persuasive?
6. Like all studies, there are limitations. The authors note several, including: “our inability to capture subjective Holocaust experiences. While our ecological definition might introduce some misclassification compared to self-reports, the latter approach also poses challenges, such as selective nonresponse and interpretive or recall biases.”
The full American Journal of Psychiatry paper can be found here:
https://psychiatryonline.org/doi/10.1176/appi.ajp.20241145
Selection 2: “AI Chatbot Use and Disclosure for Mental Health Among US Adolescents and Young Adults”
Ryan K. McBain, Jonathan H. Cantor, Joshua Breslau, et al.
JAMA Pediatrics, 1 June 2026 Online First

Since the commercial launch of artificial intelligence (AI) chatbots such as ChatGPT (OpenAI), awareness and adoption have been swiftest among adolescents and young adults. A 2025 Pew Research survey found that 64% of teens aged 13 to 17 years reported having ever used an AI chatbot… During the same period, the US has been confronting a mental health crisis among adolescents and young adults… Rates of depression (18%) and anxiety disorders (20%) among adolescents are alarmingly high. Nevertheless, 4 in 10 teenagers with a major depressive episode in the past year report not receiving mental health services, and anxiety disorders have an even larger treatment gap.
The rapid adoption of AI chatbots raises the question of how often adolescents and young adults turn to them for mental health advice. Studies conducted before the introduction of large language model (LLM)–based AI chatbots have found that adolescents frequently search for mental health information online, in part because the internet is easily accessible, anonymous, and low-cost. AI chatbots could be even more attractive as sources of advice because they offer personalized and interactive guidance.
So begins a paper by McBain et al.
Here’s what they did:
- They conducted a study to “assess the prevalence, frequency, perceived helpfulness, and disclosure of AI chatbot use for mental health advice among US adolescents and young adults.”
- To do this, they did a cross-sectional, nationally representative survey of individuals aged 12 to 21 years in November 2025 with six questions specific to AI.
- “Exposures included self-reported age, sex, race and ethnicity, census region, metropolitan status, and prior discussion with a clinician about mental health in the past 6 months.”
- Main outcome: “Self-reported use of AI chatbots for mental health advice, including any prior use, frequency of use, perceived helpfulness of responses, and disclosure of use to others.”
Here’s what they found:
- Of 1 727 individuals contacted, 1 009 responded to the survey.
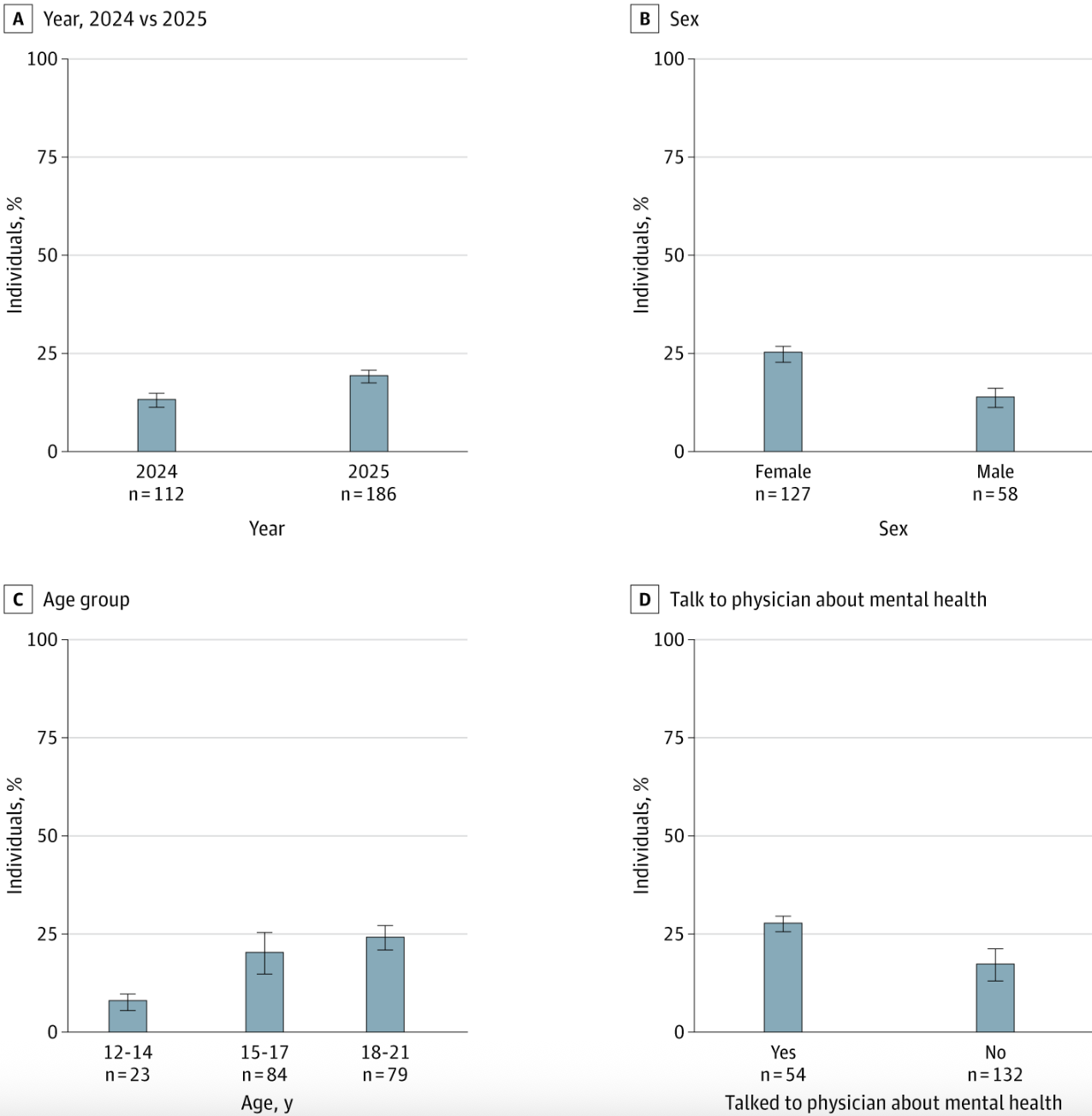
- Demographics. The US population-weighted sample included 42 825 655 youth with a median age of 17 years; many were male (50.0%) and White (49.8%).
- Use. 19.2% reported having used AI chatbots for mental health advice.
- Frequency. For those seeking advice, 42.8% did so at least monthly.
- Helpfulness. 91.7% rated the advice as somewhat or very helpful.
- Disclosure. Most adolescents reported they had not disclosed AI chatbot use for mental health advice to anyone (63.3%). (!)
- Use and demographics. It was more common among females compared with males (adjusted odds ratio [aOR], 2.10), respondents aged 18 to 21 years compared with those aged 12 to 14 years (aOR, 3.65), and those who had spoken with a physician about their mental health in the prior six months compared with those who had not (aOR, 1.89).
A few thoughts:
1. This is a good study, offering needed data.
2. The main finding in a sentence: “In this nationally representative survey, we estimated that roughly 1 in 5 adolescents and young adults in the US—representing approximately 8 million individuals—have ever used an AI chatbot for mental health advice as of 2025.”
3. Needless to say, the level of engagement suggests that AI chatbots may be filling a gap in psychological support.
4. The survey raises clinical questions. Start here: How do you talk with your patients when some could be using an AI chatbot – and may not disclose it?
5. Like all studies, there are limitations. The authors note several, including: “we did not inquire about specific AI chatbots, and we did not examine heterogeneity of respondents’ experiences and outcomes.”
The full JAMA Pediatrics paper can be found here:
https://jamanetwork.com/journals/jamapediatrics/fullarticle/2849307
Selection 3: “The Blessings and Curses of Medications”
Sarah M. Gunther
Psychiatric Services, 2 June 2026 Online First

I have spent 28 years of my life with a diagnosed mental illness. I have talked with hundreds of practitioners, have tried a dozen medications of various doses and in many combinations, and have been hospitalized twice (not including the times I was sent home with a ‘safety plan’ and a promise not to kill myself). I personally find that medication makes my life a million times easier and am eternally grateful that I was able to find the medication combination that allows me to live well. But my journey to living well was incredibly rocky.
So begins a paper by Gunther.
She talks about her first episode of illness. She was 17. “I did not know what was wrong with me: I cried for what seemed like no reason, I couldn’t make myself care about school or friends, I couldn’t concentrate, and I felt heavy and slow.”
In university, she becomes ill again. “Back then (around 2000), the psychiatrist I saw said that I could not have depression and anxiety at the same time and that I must have bipolar disorder, and she prescribed more (and different) medications. I don’t know whether it was common psychiatric practice at the time to diagnose co-occurring anxiety and depression as bipolar disorder, but the new medication combination was not as successful as the previous regimen, and I floundered quite a bit.” She describes the toll the illness takes on her life. “I withdrew from classes, waited a semester, tried again, then withdrew again. I started seeing a different psychiatrist, and the medication game was on. I now had a diagnosis of bipolar disorder, so I was taking not only antidepressants but also mood stabilizers.”
She struggles. “I spent 5 years trying medication combinations and finding solace only in alcohol, which made everything worse. In 2006 I quit drinking, but I felt broken. I was on three different medications (an antidepressant, a mood stabilizer, and a second-generation antipsychotic), and I was sleeping 14 hours a night when I was in a low mood and 3 hours when I was in a high mood. I spent most of my time in the low mood.”
She does a sleep study and is diagnosed with central sleep apnea (but it isn’t followed up). She can’t work and goes on disability. “I was either bouncing off the walls with energy or unable to get out of bed. I started working part-time for a mental health warmline but was unreliable. I was either very helpful or barely functional.”
She does her own research into sleep apnea. Could it be the antidepressant? “Well, when the sleep problems and twitches started, I had just started that one medication, the antidepressant. By this point, however, I had been taking it for almost 13 years. Surely, if the central apnea had been a side effect of the medication, someone would have caught it by now.” Should she stop it? She decides to. “My mood plummeted.”
She continues to work with her psychiatrist. “She then prescribed a different antidepressant, and I kept taking my mood stabilizer and my second-generation antipsychotic, and… I did great. I slept through the night for the first time in years. I was sleeping so soundly that my partner at the time kept poking me to see whether I was still alive. My mood swings flattened. I slept 9 hours a night consistently instead of 14 or 3 hours.”
Her life changes. “I started working full-time at a mental health nonprofit. A few years later, I had my daughter, and I now work full-time while raising her.”
“I just wish that there was a way to not have to go through years of trial and error.”
A few thoughts:
1. This is a remarkable paper. She’s had a long, difficult journey.
2. When the care isn’t a good fit: substance, unemployment, isolation. When the care works: sobriety, employment, motherhood. Wow.
3. She speaks thoughtfully about the burden on patients. “If people who are struggling with their medications could know that they can one day live as well as I do now, they would continue to try to find the right ones. But so many people never find a combination that allows them to feel well. It isn’t their fault; they have tried so many medications and dosages and combinations and still feel bad. It’s hard not to give up.” Good perspective.
The full Psychiatric Services paper can be found here:
https://psychiatryonline.org/doi/10.1176/appi.ps.20260288
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments