From the Editor
Our patients complain about the hand tremor. Some feel fatigued when they take this medication. And toxicity is always a risk.
Lithium, in other words, is tough to work with – the Callas or Pavarotti of psychotropic medications, if you will. And yet, it’s arguably the best mood stabilizer, helping people with bipolar get back their lives. Some have gone so far as to claim that all of us should take a little lithium.
Among the purported benefits of lithium: anti-suicidal effects. But does this medication really help our suicidal patients? In a new paper, Dr. Ira R. Katz (of the University of Pennsylvania) and his co-authors ask this question, armed with an impressive dataset. In a JAMA Psychiatry paper, they report the findings of a double-blinded, placebo-controlled randomized clinical trial. “The addition of lithium to usual Veterans Affairs mental health care did not reduce the incidence of suicide-related events in veterans with major depression or bipolar disorders who experienced a recent suicide event.” We consider the paper and its clinical implications.
 Lithium: the psychotropic that’s as old as the earth
Lithium: the psychotropic that’s as old as the earth
In the second selection, Dr. Tim Graham (of the University of Alberta) writes about his training and work as an ED physician, and his burnout. In a raw, highly personal essay for CMAJ, he speaks about his suicidal thoughts – and the decision to get help. He writes: “If you die tomorrow, your employer will replace you, but your loved ones cannot.” Dr. Graham also offers some practical suggestions for staying well.
DG
Selection 1: “Lithium Treatment in the Prevention of Repeat Suicide-Related Outcomes in Veterans With Major Depression or Bipolar Disorder: A Randomized Clinical Trial”
Ira R. Katz, Malcolm P. Rogers, Robert Lew, et al.
JAMA Psychiatry, 17 November 2021 Online First
![]()
Suicide is a devastating clinical and public health problem. In 2017, suicide was the nation’s 10th leading cause of death. Up to 90% of suicides are attributable to mental illness and more than 20% to diagnosed affective disorders. Veterans accounted for 13% of all US deaths from suicide in 2017, with an age- and sex-adjusted rate for all veterans 1.5 times greater than other Americans…
Several treatments are available to reduce the risk of suicidal behavior. Effective psychotherapies are cognitive-behavioral, dialectical-behavioral, and problem-solving therapies. Clozapine is approved by the US Food and Drug Administration for decreasing suicidal behavior in patients with schizophrenia and schizoaffective disorder. There is ongoing research on ketamine, and although the Food and Drug Administration recently approved esketamine for major depressive disorder and acute suicidal ideation or behavior, whether this agent is effective for preventing suicide or reducing suicidal thoughts or actions is not known. Antidepressants may be associated with reduced suicide-related outcomes in older patients but increased suicide-related outcomes in younger patients.
Numerous observational studies suggest that lithium may prevent suicide and suicide attempts in patients with bipolar disorder or depression, with some studies suggesting that this may be somewhat independent of lithium’s effects on mood. However, these observations could reflect practitioners’ propensity for prescribing lithium to patients less prone to suicide attempts. A cohort study of veterans using propensity score matching found no difference in suicide rates for patients with bipolar disorder taking lithium vs valproate. Randomized clinical trials to test whether lithium can prevent suicidal behavior in patients with bipolar disorder or depression have been underpowered…
So begins a paper by Katz et al.
Here’s what they did:
- “This double-blind, placebo-controlled randomized clinical trial assessed lithium vs placebo augmentation of usual care in veterans with bipolar disorder or depression who had survived a recent suicide-related event.”
- “Veterans at 29 VA medical centers who had an episode of suicidal behavior or an inpatient admission to prevent suicide within 6 months were screened between July 1, 2015, and March 31, 2019.”
- “Participants were randomized to receive extended-release lithium carbonate beginning at 600 mg/d or placebo.”
- The study’s main outcome is to determine the “time to the first repeated suicide-related event, including suicide attempts, interrupted attempts, hospitalizations specifically to prevent suicide, and deaths from suicide.”
Here’s what they found:
- “A total of 21 887 veterans with recent suicidal behavior or hospitalization were identified from 29 VA medical centers through electronic medical record data. Of these, 779 were eligible for and consented to a second screening, and 521 (66.9%) consented and were randomized.”
- Diagnoses. “A total of 439 (84.6%) had major depression and 80 (15.4%) had bipolar disorder, but the treatment groups were balanced.”
- Demographics. The mean age was 42.8; participants tended to be male (84.2%) and white (72.6%).
- Exposure. “Mean treatment exposure was 6.7 (4.5) months for participants with major depression and 5.6 (4.6) for participants with bipolar disorder.”
- Lithium. Mean lithium concentrations at 3 months: 0.54 mEq/L for patients with bipolar disorder and 0.46 mEq/L for patients with major depressive disorder.
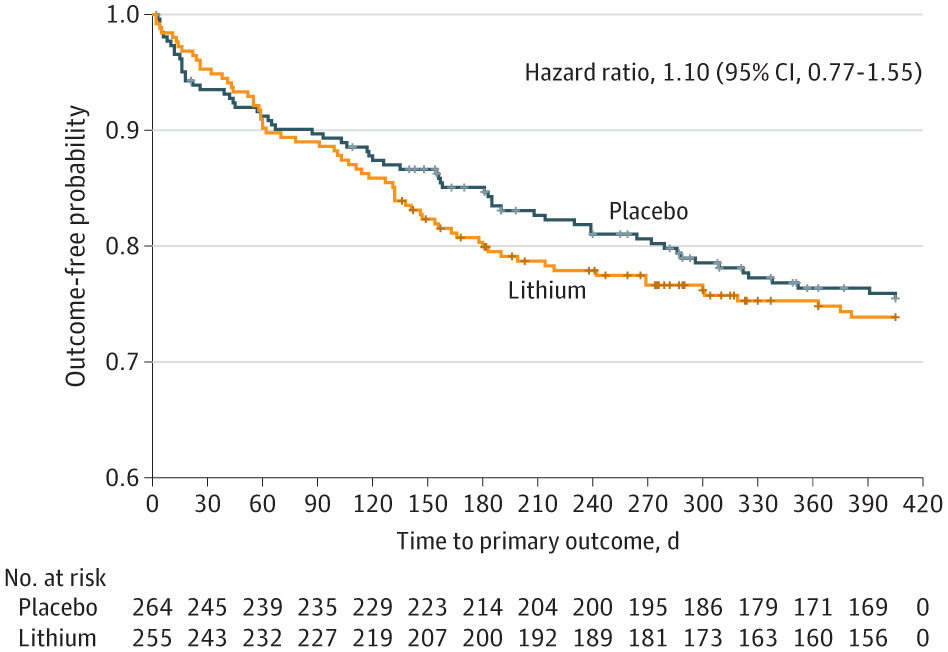
- Outcomes. “A total of 127 participants (24.5%) had suicide-related outcomes: 65 in the lithium group and 62 in the placebo group. One death occurred in the lithium group and 3 in the placebo group.”
- “The trial was stopped for futility after 519 participants were randomized.” (!!)
- “No overall difference in repeated suicide-related events between treatments was found (hazard ratio, 1.10; 95% CI, 0.77-1.55). No unanticipated safety concerns were observed.”
A few thoughts:
- This is a good study.
- There is much to like here: double-blinding, randomized, multi-centres. And, yes, the study is published in a big journal.
- How to summarize this paper? “To our knowledge, this is the largest randomized clinical trial of lithium to date that examines suicide-related behaviors as the primary outcome. Lauterbach et al and Girlanda et al studied patients with depression and found no significant effect of lithium. Oquendo et al studied patients with bipolar disorder and found no benefit of lithium over divalproex. None of these studies had adequate statistical power. The present double-blind, placebo-controlled study found no benefit of lithium over placebo for preventing or delaying suicide-related events (suicide attempts, interrupted attempts, hospitalizations to prevent attempts, or deaths from suicide) when it was added to usual VA mental health management.”
- Like all papers, there are limitations. The authors sound a note of caution: “Our findings are not necessarily generalizable to other health care settings or to other patient populations with differing proportions of individuals with bipolar disorder, lower rates of comorbidities, or higher treatment adherence.”
- But is this paper persuasive? Drs. Ross J. Baldessarini and Leonardo Tondo (both of Harvard University) respond in an editorial, “Testing for Antisuicidal Effects of Lithium Treatment.”
 Ross J. Baldessarini
Ross J. Baldessarini
They have serious reservations about the study, particularly about the lithium levels.
A particularly important limitation of the study is the low circulating concentrations of lithium, with a mean level of 0.54 mEq/L (to convert to millimoles per liter, multiply by 1) among the 15.4% of participants diagnosed with bipolar disorder and an even lower level of 0.46 mEq/L among the most participants (84.6%) diagnosed with major depressive disorder; less than 50% reached a lithium level of 0.5 mEq/L. Moreover, adherence to prescribed lithium or placebo was considered adequate in only 17.0% of participants, and 68% of participants treated with lithium correctly guessed this assignment. Treatment exposure was brief (38.4 weeks), with modest numbers of participants randomized to adjunctive treatment with lithium (n = 255; 144 retained for 1 year) or a well-matched placebo (n = 264; 125 retained for 1 year), with many early dropouts (51.6% of 521 randomized).
The editorial can be found here:
https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2786430
- Drs. Baldessarini and Tondo are well established in this field – but are their comments a bit too strong? The final conclusion of Katz et al. is quite reasonable and clinically relevant: “simply adding lithium to existing medication regimens is unlikely to be effective for preventing a broad range of suicide-related events in patients who are actively being treated for mood disorders and substantial comorbidities.”
- Of course, even if you could conclude that lithium doesn’t have anti-suicidal effects, there are good reasons to prescribe this medication. Past Readings have considered lithium, including the Bohlken et al. paper suggesting better compliance: https://davidgratzer.com/reading-of-the-week/reading-of-the-week-lithium-vs-newer-meds-for-bipolar-whats-best-also-nudging-vaccines-and-beale-on-her-illness-experience-being-a-doctor-bmj/
The full JAMA Psychiatry paper can be found here:
https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2786428
Selection 2: “Physician, heal thyself”
Tim Graham
CMAJ, 18 October 2021

In my two decades of emergency medicine practice, I have encountered many patients who have attempted suicide by medication overdose. Most attempts seemed impulsive, with a poor understanding of the lethality of the drugs taken. When my own suicidal thoughts got out of control, I found myself relying on my medical training to calculate a lethal dose.
During residency, I was proud of being able to manage stress. But when newly hired into a large teaching hospital, I found myself struggling to keep up with the intense work and plagued by self-doubt regarding my knowledge base and skills compared with my colleagues. A lack of ability to cope with these feelings was the first inkling of a long, steady decline that would deeply affect my life and those around me.
So begins a paper by Dr. Graham.
He notes the lack of training around wellness: “Almost none of my training time in the late 1990s was spent on the wellness and resilience skills that are now commonly taught. None of my colleagues or mentors – and I had some great ones – mentioned self-care. The only skill I mastered to deal with the increasing stress was denial.”
Over time, his mental health suffered: “By my late thirties, things had gradually deteriorated and I experienced progressive burnout, with symptoms such as sleep disruption, irritability, poor concentration and lack of empathy for my patients…”
“I dreaded going to work.”
He goes into detail on his symptoms and the decision to start antidepressants (coloured by side effects). “Eventually, I internalized the thought that my wife and three children would simply be better off without me. It seemed my cycle of listlessness, hopelessness, anxiety, feelings of incompetence and worthlessness would continue indefinitely, and my suicidal thoughts started to coalesce into a plan. My medicine cabinet had full bottles of bupropion, two SSRIs, zopiclone, post-wrist-surgery oxycodone, ibuprofen, acetaminophen (all promising) and a salbutamol inhaler (useless). None would be fatal on its own but, I was pretty sure, as I calculated dosing, I would be unlikely to survive if I took them all with conviction. One day, I started finalizing my doses and calmly thinking through the logistics…”
“It was an image of one of my children finding me on the floor that stopped me.”
Fortunately, he received care, and got better: “After much help, self-reflection and self-care, I am off medications and consider myself to be in remission – not cured – of my illness. My monkey mind is all too willing to chime in with negative and melancholic thoughts.”
A few thoughts:
- This is a bold and important paper. It’s tough for anyone to speak of their mental health struggles; it’s exceptionally rare for a physician to do so.
- Are there lessons to learn here? Dr. Graham closes with a few thoughts, including the helpfulness of a support network. This comment is important:
I would highly encourage my younger self to develop a toolkit for health that emphasizes sleep hygiene, physical exercise, a healthy diet and, most critically, a mental health practice that includes meditation. Books like Why We Sleep, by Andrew Walker, outline the incredible physical and mental health consequences of poor sleep, and strategies to improve it. In high school or university, my peers would probably have voted me least likely to ever practise meditation or yoga, but there are important lessons in a meditation practice that give insight into managing stress and anxiety, and it is not hyperbole to say they have radically improved my life. Mobile applications such as Waking Up or Headspace make learning meditation easy, and managing my thoughts and emotions is now a fundamental pillar of my self-care.
- CMAJ doesn’t often publish essays like this. I note that Dr. Graham’s paper has had more than 30 000 reads on that journal’s website in October. (!!)
The full CMAJ paper can be found here:
https://www.cmaj.ca/content/193/41/E1601
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
November 27, 2021 at 2:57 am
Thank you for sharing your experience!