From the Editor
“Mental illness may have been a factor.”
It’s just seven words, but they so often accompany reports of mass murder. And psychosis is mentioned more often than not. The message is clear: mental disorders, particularly psychotic disorders, are highly tied to violence.
In the first selection, we look at a new paper that reviews 120 years worth of mass murder, and distinguishes between gun violence and non-gun violence. Just published in Psychological Medicine, Gary Brucato (of Columbia University) and his co-authors have written an extraordinary paper. They also reach an important conclusion: “These results suggest that policies aimed at preventing mass shootings by focusing on serious mental illness, characterized by psychotic symptoms, may have limited impact.” We look at the big paper.

In the second selection, from The Lancet Psychiatry, Dr. Livia J. De Picker (of the University of Antwerp) and her co-authors consider European countries and vaccination prioritization, with a focus on mental disorders. “Only four countries (Denmark, Germany, the Netherlands, and the UK) had some form of higher vaccination priority for outpatients with severe mental illness.”
And, in the third selection, writer Andray Domise considers mental illness and medical assistance in dying. In a personal essay for The Globe and Mail, he raises objections. Start here: he would have opted to die when he was unwell. He argues the whole legislative approach is wrong: “This is a country that continues to fail in respecting the humanity of people with disabilities. And rather than find strength of character to improve ourselves, the Canadian government is set to fall back on egregious historical precedent by offering death instead.”
DG
Selection 1: “Psychotic symptoms in mass shootings v. mass murders not involving firearms: findings from the Columbia mass murder database”
Gary Brucato, Paul S. Appelbaum, Hannah Hesson, et al.
Psychological Medicine, 18 January 2021 Online First

Mass murder has generally been defined as the unlawful killing of four or more individuals, excluding the perpetrator(s), within one event, in one location. In 2013, the US Congress proposed the alternative parameter of three or more victims. In the USA, mass murders involving firearms, commonly termed mass shootings, have become more prevalent, with greater numbers of casualties, since 2000, and especially since 2010. Although mass shootings account for only a small fraction of the murders committed annually in the USA or worldwide, they exert a disproportionately strong influence on society, invoking collective fear and calls for preparedness and policy changes. This growing public health concern has prompted calls for discourse and research regarding the relationship between mass shootings and mental illness, with potential implications for the stringency of state firearm laws and other policy changes that might aid prevention.
Depending on the definition of mental illness used, the proportion of mass shootings associated with it varies from 4.7% to 78% across studies. Silver, Simons & Craun reported that 25% of 63 active shooters identified by the Federal Bureau of Investigation (FBI) had psychiatric disorders. Among the perpetrators of 167 mass shootings in the USA between 1966 and 2019 analyzed for The Violence Project, 19% had previously been hospitalized for psychiatric reasons; 25% had undergone counseling; 20% had used psychotropic medications; 23% had mood disorders; and 26% exhibited thought disorders. Psychosis was at least a partial motivating factor in 15.8% of cases. Stone found that 22% of mass murderers were mentally ill.
So begins a paper by Brucato et al.
Here’s what they did:
- Drawing on various databases, they examined global personal-cause mass murders from 1900 to 2019, amassed by review of 14 785 murders publicly described in English in print or online.
- “Personal cause” means those motivated personally – that is, not occurring within the contexts of war, terrorism, or organized crime.
- They collected information regarding the perpetrator, demographics, legal history, drug use and alcohol misuse, and history of symptoms of psychiatric or neurologic illness using standardized methods.
- They distinguished whether firearms were or were not used, and, if so, the type (that is, non-automatic versus semi- or fully-automatic).
- Statistical analyses were done.
Here’s what they found:
- They identified 1315 mass murders, with 10 877 fatalities. (!)
- The vast majority (65%) involved firearms.
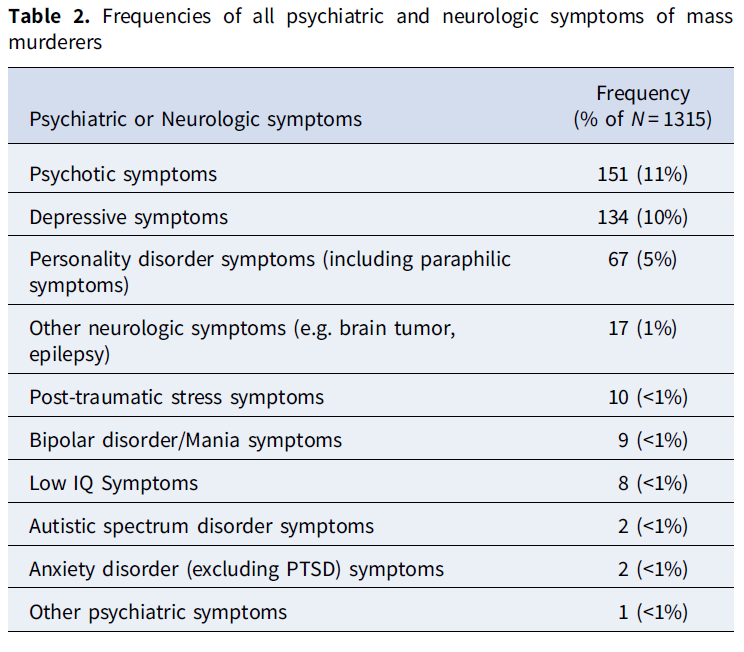
- “Lifetime psychotic symptoms were noted among 11% of perpetrators, consistent with previous reports, including 18% of mass murderers who did not use firearms and 8% of those who did (χ2 = 28.0, p < 0.01).”
- See table below for diagnoses.
- “US-based mass shooters were more likely to have legal histories, use recreational drugs or misuse alcohol, or have histories of non-psychotic psychiatric or neurologic symptoms. US-based mass shooters with symptoms of any psychiatric or neurologic illness more frequently used semi-or fully-automatic firearms.”
The authors note: “In accord with our hypothesis, we found that mass murderers who used firearms were significantly less likely to have a lifetime history of psychotic symptoms than mass murderers who use other methods: 18% of mass murderers who did not use firearms had a history of psychotic symptoms, compared to 8% of mass shooters.”
- This is an impressive study drawing on more than a century of data.
- So much for the media depiction – psychosis wasn’t so common. Is media commenting on mental illness another example of stigma and bias?
- How do the findings compare to other studies? As the authors note, they compare well to other studies, such as the Parks et al. report that focused on the United States. Of course, it’s a matter of definitions here: the Brucato et al. paper defines mental disorders in terms of major illness, not, say, casual drug use.
- Limitations? The authors note that diagnoses are often drawn from less reliable sources, including court documents.
- Circling back to the conclusion: “policies aimed at preventing mass shootings by focusing on serious mental illness, characterized by psychotic symptoms, may have limited impact.” That comment seems reasonable with significant public policy implications for mental health policy, yes, but also gun control.
The full paper can be found here:
Selection 2: “Severe mental illness and European COVID-19 vaccination strategies”
Livia J. De Picker, Marisa Casanova Dias, Michael E Benros, et al.
The Lancet Psychiatry, 17 February 2021 Online First
![]()
The EU advises prioritising vaccination for people whose health makes them particularly at risk for severe COVID-19, but leaves it to member states to decide which medical conditions get prioritised. Ethical, neuroscientific, and public health considerations have been used to prioritise individuals with severe mental illness (ie, psychotic disorders, bipolar disorders, and severe major depressive disorders). We systematically reviewed national COVID-19 vaccine deployment plans across 20 European countries.
Eight of 20 countries explicitly mentioned psychiatry or mental illness in their national vaccine strategy documents. Several countries prioritised institutional residents, which can include people with severe mental illness. Only four countries (Denmark, Germany, the Netherlands, and the UK) had some form of higher vaccination priority for outpatients with severe mental illness. Additionally, Latvia, Romania, Spain, and Sweden prioritised outpatients with disabilities, possibly including severe mental illness, whereas the Czech Republic and Sweden specified behavioural or mental problems interfering with pandemic regulation adherence as priority indication.
So begins a paper by De Picker et al.
The authors focus on these four countries and their decision making:
- United Kingdom. The government drew on “an Oxford University evidence-based algorithm to calculate the number of vaccinations needed to prevent one death. Importantly, this QCovid algorithm, based on UK data from Jan 24 to June 30, 2020, explicitly includes severe mental illness among its risk predictors, and so does the UK vaccination strategy.”
- Denmark and the Netherlands. These two countries “initially omitted mental disorders from their COVID-19 vaccination strategies.” But “after a large nationwide Danish cohort study found that an increased risk for 30-day mortality was associated with severe mental illness (adjusted OR 2·5) and use of antipsychotics (adjusted OR 3·3), the Danish Health Authority urged health-care practitioners to refer for priority vaccination patients with psychotic disorders and other individuals with complex severe mental illness deemed to be at particularly high risk by the treating physician.” The Netherlands also changed its position after lobbying from mental health groups.
- Germany. “Following an update of its literature review, in which severe mental illness was found to be one of the few medical comorbidities with OR more than 2·0 for COVID-19 hospitalisation and mortality, the new strategy now explicitly includes severe mental illness in the highest risk group of medical comorbidities.”
A few thoughts:
- This is a short but relevant paper.
- Though all countries are dealing with the same problem, approaches differ. The decision of these four European nations is evidence based.
- Last week, Toronto announced that people who are without stable housing are eligible for phase 1, allowing them to receive vaccination starting on Monday. Other jurisdictions have weighed a similar move. It’s a step in the right direction. Not everyone in that population has mental illness, but the vast majority do.
- But why aren’t we prioritizing more people with mental illness here in Canada? Should we follow the lead of these four nations?
The paper can be found here:
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(21)00046-8/fulltext
Selection 3: “Canada’s proposed expansion of assisted-death threatens to push the mentally ill out the door”
Andray Domise
The Globe and Mail, 13 February 2021

Last spring, a few months into Ontario’s initial COVID-19 lockdown, I suffered the worst anxiety attack I’d had in years, requiring medical intervention. I’ve experienced these kinds of episodes since my early 20s, with the most severe ones forcing me to relive repressed and traumatic memories as if they’ve just happened. In the past, they’ve led to intense bouts of suicidal ideation that can last for days at a time, with echo effects that can last months.
I was only properly diagnosed and provided medical attention for this and other conditions in my mid-30s – meaning that, for more than a decade, my mind periodically attempted to destroy itself and the body carrying it, and I wasn’t getting any help or support. And even when I received the diagnosis and treatment I needed, I’ve experienced the sort of financial instability that forced me to choose between taking time off work for adequate recovery and maintaining the ability to live independently and feed myself.
So if an option for ending my life with the assistance of medical professionals had existed back then, I would likely be dead today.
So begins an essay by Domise.
He notes his good fortune in recent years, with a family and financial security. Yet, others aren’t so lucky. “Poverty and disability are inextricably linked in our society, even for those of us who are mostly or even fully able-bodied. The alarming rates of suicide among Black and Indigenous people only confirm that I’m one of the lucky ones.”
He continues: “I mention this because the Canadian government is on the cusp of pushing through Bill C-7, which would expand access to medical assistance in dying (MAID) with a broad enough scope to give people diagnosed with ‘serious and incurable illness, disease or disability’ and an ‘irreversible decline of capabilities’ the option to end their lives, even when natural death due to such disability isn’t foreseeable. The Senate has even amended Bill C-7 to open the door for MAID to be offered to people with solely mental illnesses. It has also nixed a failsafe to prevent medical professionals from suggesting MAID as an option if it wasn’t first raised by the patient.”
He is concerned: “The expansion of MAID shows a side of Canada that is anything but merciful. And despite the insistence of well-heeled advocates, there is nothing dignified about this approach. It is a gruesome reminder of our tendency to pat ourselves on the back for thinking Canada is a progressive nation, even as our legacy of eugenics continues to haunt us.”
“We laud our progressive approach to ‘dignity in death,’ even while the United Nations stands alarmed at the potential for ‘subtle pressure’ being applied through ‘lack of services or lack of community living options’ in such legislation. We see Indigenous peoples in the grip of a suicide crisis but, according to Denesuline elder François Paulette, consultation with their communities was apparently too much to ask for.”
He notes the opposition: “They’ve made it clear that disability is not the problem, but the way society views and treats disability. And yet this bill is being pushed through anyway.”
A few thoughts:
- This is a forceful essay.
- The debate over mental illness and MAiD divides people. Domise makes good points – and makes the essay very personal.
- Of course, others disagree. In that newspaper, columnist André Picard argued in favour of expansion in an earlier essay. Here’s the link: https://www.theglobeandmail.com/opinion/article-canadians-with-mental-illness-deserve-access-to-medical-assistance-in/
- Regardless of personal views on MAiD and mental illness, Bill C-7 could have a major impact on the mental health care. How would we address the requests of those who want MAiD?
- Domise opens personally by talking about his problems and the decisions he may have made if MAiD were more accessible at that time. Both sides on this debate should be given pause by his comments and seek to answer an important question: What safeguards must be put in place?
The Domise essay can be found here:
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments