From the Editor
Though years had passed since his peacekeeping service in Bosnia, my patient lucidly described the flashbacks and nightmares that still haunted him. It raises an important question: is it possible to prevent PTSD in the first place?
In a new, important American Journal of Psychiatry paper, Chelsea Dyan Gober Dykan (of Tel Aviv University) and her co-authors attempt to answer that question by drawing on past work showing the effectiveness of response-time-based attention bias modification (RT-based ABM), a cognitive training technique. They describe a three-arm randomized controlled trial involving more than 500 male combat-bound soldiers who, before combat exposure, received one of two cognitive training techniques (RT-based ABM and a variant focused on gaze) or a sham intervention. Participants then reported on PTSD symptoms after it. “Consistent with a previous randomized controlled trial, RT-based ABM reduced risk for PTSD relative to sham ABM when implemented prior to combat exposure.” We consider the paper and its implications.

How common are AI hallucinations? In the second selection, Jake Linardon (of Deakin University) and his co-authors look at hallucinations through the prism of psychiatry, asking ChatGPT to draft writing on several disorders. In their JMIR Mental Health study, hallucinations were frequent. “Citation fabrication and bibliographic errors remain common in GPT-4o outputs, with nearly two-thirds of citations being fabricated or inaccurate.”
Finally, in the third selection from Academic Psychiatry, Dr. Sheba Gollapudi (of the University of Texas) mulls the power of the stethoscope and its psychiatric equivalent. She describes how she developed her listening skills and her use of silence. “Because even though I will not necessarily use a stethoscope in my everyday practice, I know now that the stethoscope is within me.”
DG
Selection 1: “Primary Prevention of PTSD Symptoms in Combat-Deploying Soldiers Using Attention Bias Modification: A Randomized Controlled Trial”
Chelsea Dyan Gober Dykan, Yoav Levinstein, Lucian Tetse-Laur, et al.
The American Journal of Psychiatry, 18 November 2025 Online First

Primary prevention of posttraumatic stress disorder (PTSD) aims to reduce symptom risk by intervening before trauma exposure… Attention bias modification (ABM) shows promise in targeting attentional threat avoidance and reducing PTSD risk in combat-bound soldiers. Although attentional threat avoidance may provide short-term relief, it has been linked to greater long-term PTSD, depression, and anxiety severity. Integrating evidence linking threat avoidance to PTSD risk, preventive ABM trains soldiers to direct attention toward threat-related stimuli. A randomized controlled trial (RCT) suggested that ABM delivery immediately before combat disrupts the common association between combat exposure and PTSD symptoms. In another RCT, ABM delivered before combat was found to reduce PTSD risk 4 months postcombat relative to no training.
To manipulate attention toward threat, response-time (RT)-based protocols have used the dot-probe task with targets presented with high probability at the location of threat over neutral stimuli. The assumption is that participants implicitly learn the contingency between threat and target location and use it to enhance performance. A recently developed eye-tracking-based ABM method, called gaze-contingent music reward training (GC-MRT), uses feedback and operant conditioning principles. GC-MRT combines gaze-tracking with music rewards to train gaze behavior. Evidence supports GC-MRT’s efficacy in reducing threat-related attention biases and anxiety symptoms, along with strong reliability in measurement. However, GC-MRT has not yet been applied to PTSD treatment or prevention.
So begins a paper by Dykan et al.
Here’s what they did:
- They conducted a “three-arm RCT [which] tested RT-based ABM and GC-MRT against sham control as primary prevention of PTSD in combat-bound soldiers.”
- In terms of the interventions, participants did four sessions of active or sham interventions during a three-month period of advanced combat training before any combat exposure.
- Participants’ first combat deployment was in January 2022.
- “Threat-related attention was measured before and after training.”
- Primary outcome: self-reported symptoms of PTSD.
Here’s what they found:
- 570 were contacted with 501 randomized as follows: RT-based ABM (N = 164), GC-MRT (167), and sham RT-based control (170).
- Demographics and past trauma. The mean age was 19.49 years, and all participants were male. The groups did not differ significantly in pre-military traumatic experiences.
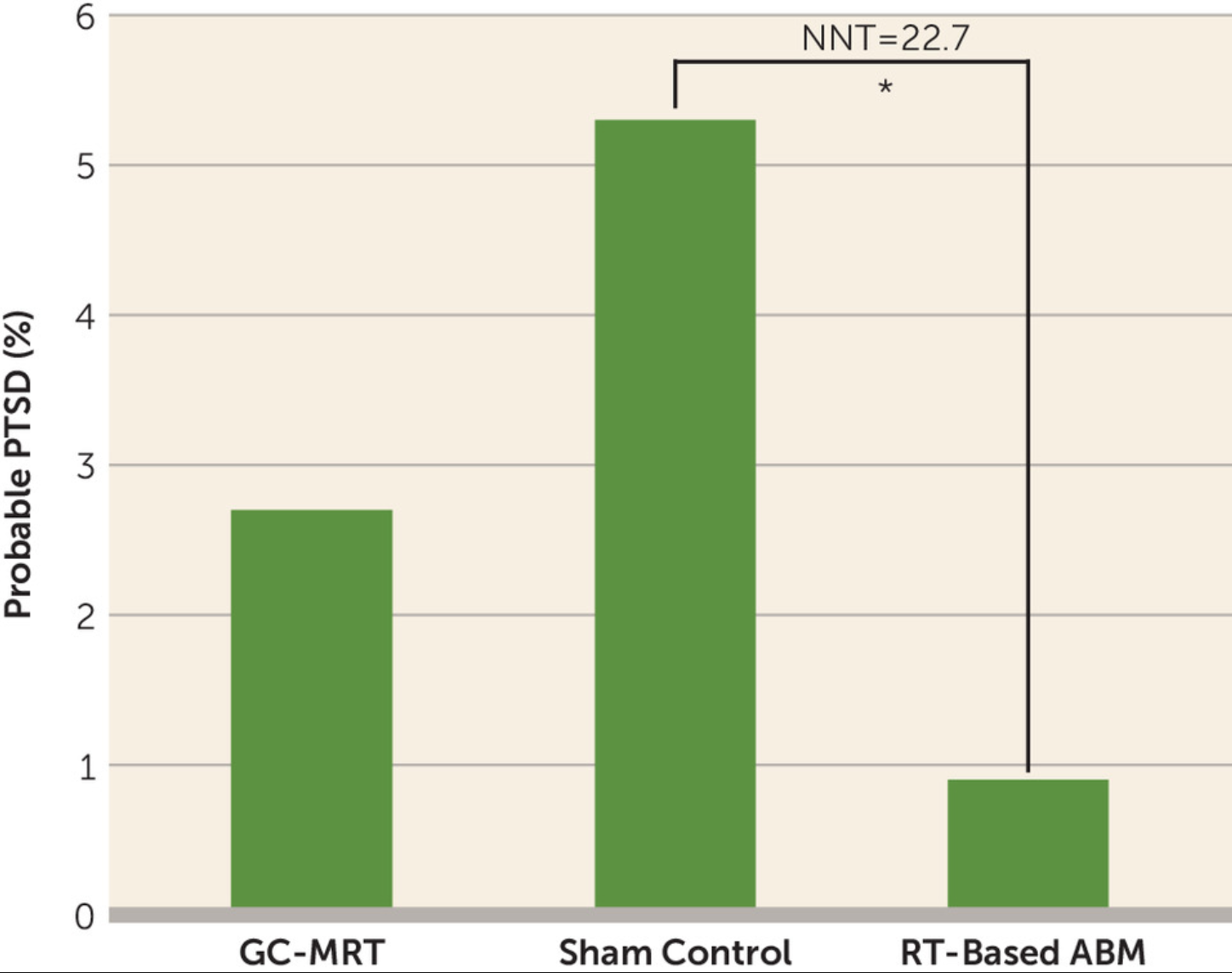
- Symptoms – RT-based ABM. This cognitive training technique was associated with “lower symptom severity and lower prevalence of probable PTSD postcombat relative to sham training (number needed to treat=22.7).” See figure below.
- Symptoms – GC-MRT. This other cognitive training technique didn’t result in statistically significant PTSD symptoms from the sham control group.
- Attrition. 73% of the participants completed the post-combat assessment.
A few thoughts:
1. This is an impressive study – an RCT with solid data and a sham comparison – and published in a major journal.
2. The key findings in a sentence: like past work, the results supported “the efficacy of RT-based ABM as a prevention for PTSD delivered prior to combat exposure” – but not that of GC-MRT.
3. Wow.
4. The core idea here: RT-based ABM trained participants to direct attention toward threat-related stimuli instead of avoiding them. Interesting. (Obviously the paper offers a more complete explanation, including pictures.)
5. By the standards of medicine, a NNT of 22.7 is good. To phrase things differently, for every twenty soldiers trained, one didn’t develop PTSD.
6. The authors see clear clinical implications: “the demonstrated replicable efficacy of RT-based ABM highlights its potential for widespread implementation in military training programs as a preventive measure against PTSD in combat-bound troops.” That said, they do offer a note of caution: “The modest effect sizes and the number needed to treat values indicate that although potentially beneficial, RT-based ABM should probably be integrated as part of a comprehensive resilience-building framework rather than a stand-alone solution.”
7. Like all studies, the authors note several limitations, including: the self-reporting of symptoms.
The full AJP paper can be found here:
https://psychiatryonline.org/doi/10.1176/appi.ajp.20250160
Selection 2: “Influence of Topic Familiarity and Prompt Specificity on Citation Fabrication in Mental Health Research Using Large Language Models: Experimental Study”
Jake Linardon, Hannah K. Jarman, Zoe McClure, et al.
JMIR Mental Health, 12 November 2025

“Large language models (LLMs) are a class of tools gaining traction in academic settings to support researchers. LLMs are advanced artificial intelligence systems trained on vast amounts of textual data to generate coherent and contextually relevant natural language responses… A recent study showed that nearly 70% of mental health scientists reported using ChatGPT to assist with research-related tasks, including writing and drafting, coding, and administrative support. However, while most LLM adopters reported that these tools enhanced research efficiency and improved the quality of their work, many also expressed concerns about inaccuracies… One type of hallucination generated by LLMs that has received increasing attention among researchers is fabricated bibliographic citations that cannot be traced to existing scholarly publications…
Recent work has sought to quantify the extent of these hallucinations, typically by analyzing the citations produced when LLMs are prompted to generate academic literature reviews on specific topics. Walters and Wilder prompted GPT-3.5 and GPT-4 to generate short literature reviews on 42 multidisciplinary topics and found that 55% and 18% of the citations, respectively, were fabricated, and 43% (GPT-3.5) and 24% (GPT-4) of the real citations contained substantive errors…
So begins a paper by Linardon et al.
Here’s what they did:
- They prompted GPT-4o to generate six literature reviews (2 000 words with 20 or more citations) on three mental disorders “representing different levels of public awareness and research coverage…” The disorders: major depressive disorder, binge eating disorder, and body dysmorphic disorder.
- For each disorder, they requested a general overview (symptoms, impacts, and treatments) and a specialized review (evidence for digital interventions).
- The citations were extracted and verified. They then classified citations as “fabricated (no identifiable source), real with errors, or fully accurate.”
- “Fabrication and accuracy rates were compared by disorder and review type by using chi-square tests.”
Here’s what they found:
- GPT-4o generated 176 citations.
- Quality. 19.9% were fabricated. Among the real citations, 45.4% contained errors (most frequently incorrect or invalid digital object identifiers).
- Disorders. Fabrication rates differed significantly by disorders with higher rates for binge eating disorder (28%) and body dysmorphic disorder (29%) than for major depressive disorder (6%).
- Accuracy. Rates also varied by disorder being lowest for body dysmorphic disorder (59%) and highest for major depressive disorder (64%).
A few thoughts:
1. This is an interesting and relevant paper on a timely topic.
2. The main findings in a sentence: “A total of 35 (19.9%) citations were fabricated, and among the 141 nonfabricated citations, 77 (54.6%) contained bibliographic errors, with incorrect DOIs being the most prevalent error type.” To add more detail: Fabrication and accuracy rates varied by disorder.
3. Ouch.
4. We hear often about AI hallucinations. This paper provides a unique perspective, offering data on mental disorders. Note that ChatGPT did better with a more common illness (major depressive disorder) than a less common one (body dysmorphic disorder).
5. The authors see implications for researchers, cautioning them to carefully check AI-generated citations. Fair. They also worry about the scholarly standards of academic journals and urge editors to employ AI detectors. (A very 2025 point.)
6. Like all studies, there are limitations. The authors note several, including the lack of generalizability: “although a key strength of this study was the manipulation of topic complexity and public familiarity within a single domain, the findings may not generalize to other psychiatric disorders or specialized subfields not examined here.”
7. Past Readings have considered AI and mental health. In September, the selections included a paper by Dr. Andrew Clark (of Boston University) looking at AI chatbots responses to clinical situations. “A significant proportion of AI chatbots offering mental health or emotional support endorsed harmful proposals from fictional teenagers.” That paper can be found here:
https://davidgratzer.com/reading-of-the-week/reading-of-the-week-ai-therapy/
The full JMIR Mental Health paper can be found here:
https://mental.jmir.org/2025/1/e80371
Selection 3: “Human Stethoscope”
Sheba Gollapudi
Academic Psychiatry, 8 September 2025 Online First

When I was a little girl, my grandmother would tell me that she was looking forward to seeing me become a doctor, wearing my stethoscope. Years later, after I had gotten into medical school, I had taken a picture of myself wearing my white coat, but she specifically wanted a picture of me with my stethoscope. I got around to taking the new picture eventually, but it was not long after this that she passed away. To this day, I am not sure if she actually saw that picture before she left us, and I still feel a little guilty about it.
Truth be told, I was not upset about having to leave my stethoscope behind when I decided to become a psychiatrist. It always felt so heavy around my neck! But I can understand why the stethoscope carries so much significance.
So begins a paper by Dr. Gollapudi.
She comments on the significance of the tool: “the stethoscope gives us the ability to listen to what is on the inside. It is how we might first learn that something is wrong, which then helps us figure out how to approach the next steps.”
She mulls the psychiatric equivalent. “I learned that listening is one of the most powerful diagnostic and therapeutic tools I could possess, and I began to more deeply appreciate my role as a doctor in being with a patient – not just doing something for a patient. Many times, I would start to feel helpless after hearing my patients share their difficult stories with me – especially if there was nothing I could do to more immediately solve their problems. I felt that I should have been able to do more, with all the knowledge and skills I had gained thus far. But when my patients would say, ‘Thanks for listening,’ or, ‘Thanks for hearing me out,’ I realized that just being with them in the moment was more healing than finding the right medication to prescribe or the right referral to place.”
She discusses her outpatient years of training when “I learned – perhaps the hard way – that it is sometimes better to listen than give advice.” With one patient who “shared with me that she was feeling down, in the context of various stressors, I was eager to pull out some acceptance and commitment therapy skills. Even if we could not change some of these problems right now, how could we go about supporting her in finding ways to still live a meaningful life?” The response is surprising to the young doctor: “she became somewhat frustrated and asked why she could not just be allowed to experience her emotions. It gave me a lot to think about, and over time, I shifted towards more reflective listening in my appointments with her.”
Dr. Gollapudi remembers a psychodynamic psychotherapy patient. “There were moments when I intentionally refrained from asking or saying anything. Sometimes this resulted in what felt like an awkwardly long silence, and at other times this resulted in the patient going on what felt like a tangent. But I began to see that it was out of my own silence that the most poignant thoughts and emotions might then emerge from him.”
With her residency drawing to a close, she adds: “I am grateful for having learned the art of listening and for appreciating its true power.” Thinking about her career ahead, she writes: “I will know how to listen to my patients well, and I know that this will go a long way. As one of my supervisors often says, ‘The patient is your best supervisor,’ and this is something I hope to model for our next generation of medical students and residents, as I continue working with them in clinical settings.”
“As I reflect on my experience in training, then, I hope that I have still made my grandmother proud.”
A few thoughts:
1. This is a well-written essay on training and skills.
2. She vividly describes the importance of stethoscopes in the image of physicians – and their lack of importance in the clinical work of most psychiatrists.
3. And she beautifully examines the power of silence and pauses.
The full Academic Psychiatry paper can be found here:
https://link.springer.com/article/10.1007/s40596-025-02201-y
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments