From the Editor
“The pain in my feet. It’s killing me.”
That’s what John told me when I asked him what he needed help with. It’s not quite the answer I thought he’d give – John has schizophrenia and he has significant side effects from his medications. But, like many people with mental illness, he also struggles with physical illness (diabetes and the accompanying neuropathy).
Many of our patients have both physical and mental illnesses. When faced with these twin challenges, how do they fair?
In this week’s first selection, we look at a new paper that considers people with schizophrenia and diabetes. The study authors find a significant gap between the care received by those with and without mental illness.
 An old drug, an old illness, and a big problem for those with mental illness
An old drug, an old illness, and a big problem for those with mental illness
In our second selection, drawing from a lively blog written by medical student Ali Damji, we look at Swedish health care.
DG
Diabetes and Care
“Diabetes quality of care and outcomes: Comparison of individuals with and without schizophrenia”
Paul Kurdyak, Simone Vigod, Raquel Duchen, Binu Jacob, Thérèse Stukel, Tara Kiran
General Hospital Psychiatry, May-June 2017 (Published Online First)
http://www.sciencedirect.com/science/article/pii/S0163834316303711

Diabetes is common among individuals with schizophrenia, with a median prevalence rate of 13%, and documented prevalence rates as high as 50%. Diabetes is more common among individuals with schizophrenia than among those with other mental illnesses, and much more common than in the general population. Individuals with schizophrenia have more diabetes risk factors such as obesity, poor diet, and reduced physical activity relative to individuals without schizophrenia. Additionally, second-generation antipsychotics, a mainstay of treatment for schizophrenia, contribute to the high prevalence of diabetes through weight gain and insulin resistance. The substantial mortality gap between individuals with and without schizophrenia is largely explained by an increase in cardiovascular deaths, for which diabetes is a significant risk factor.
Careful monitoring of blood pressure, cholesterol and glycemic control reduce morbidity and mortality for individuals with diabetes, and diabetes care guidelines have been developed in multiple jurisdictions to encourage optimal care. When diabetes is comorbid with schizophrenia, there are patient, provider, and system-level factors that make it challenging to follow evidence-based guidelines. Patients with schizophrenia have a significant level of cognitive disorganization and social instability that makes engaging in care difficult. Providers may be overwhelmed by the complexity and may not have the time or resources needed to provide optimal care. Finally, mental health care and primary care can be fragmented and there is relatively little evidence on how to design care that involves multiple health care providers when one of the comorbidities is a serious mental illness.
 Paul Kurdyak
Paul Kurdyak
So begins a paper by Kurdyak et al. that uses a retrospective cohort study to compare the diabetic care of those with schizophrenia and diabetes, and those with only diabetes.
Here’s what they did.
- The authors drew data from several databases covering different aspects of health service delivery including the Ontario Health Insurance Plan (outpatient physician billing, as well as diagnostic codes and procedures) and CIHI Discharge Abstract Database (acute hospitalizations).
- The participants were adults eligible for the Ontario Health Insurance Plan, with the study covering a period of two years, from April 1, 2011.
- Diabetic care was based on participants getting the care recommended by the Canadian Diabetes Association 2013 Clinical Practice Guidelines – at least 4 Hb1AC tests, one cholesterol test, and one retinal exam.
- They looked at demographic information, and other co-variables: residential instability, maternal deprivation, etc.
- Statistical analysis was done, including an ANOVA analysis.
Here’s what they found:
- On April 1, 2011, there were 1,131,415 individuals with diabetes age 19 to 105; of these, 26,259 (or 2.3%) had schizophrenia.
- Demographically: those with schizophrenia were significantly more likely to be female and younger. They were significantly more likely to live in an urban setting, and in lower income neighbourhoods.
- In terms of health care use: individuals with schizophrenia were more likely to use health care: they were more likely to have at least one ED visit for a diabetes complication (8.1% vs. 5.9%), and at least one ED visit for any reason excluding trauma (55.5% vs. 40.2%), and to be hospitalized for a diabetes complication (6.0% vs. 4.7%).
- In terms of diabetic care: “Individuals with schizophrenia were less likely to receive guideline-level screening for diabetes.” They received the recommended number of cholesterol tests less than those without schizophrenia (72.4% vs. 80.3%) and the recommended number of eye exams (56.8% vs. 67.4%). “There was a smaller, but significant difference in the proportion of individuals who received the recommended number of HbA1c tests between the two groups (35.8% vs. 37.7%…).”
- In terms of an adjusted odds ratio: “Individuals with schizophrenia were less likely to be guideline-concordant with one of the 3 recommended tests (aOR = 0.84 95% CI 0.81–88), two tests (aOR = 0.71 95% CI 0.68–0.74) and three tests (aOR = 0.60 95% CI 0.57–0.62) in comparison to individuals without schizophrenia.” See the following graph:
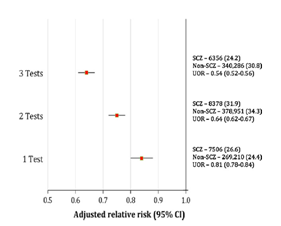
They note:
They also have approximately 30% more visits with their primary care physician. Despite this frequent primary care contact, individuals with schizophrenia are less likely to have cholesterol testing and eye exams, and are one third less likely to receive all three guideline-based tests (HbA1c, cholesterol testing and eye exams). Finally, individuals with schizophrenia are about one third more likely to have diabetes-related hospitalizations and ED visits.
The authors go on to consider ways that diabetic care could be improved for those with major mental illness. They note evidence in the literature for co-location of specialists, as well as the use of diabetic nurses in primary care.
A few thoughts:
- This is a good study. It speaks to the gap in care – but, at the same time, the strikingly high costs of that gap (greater utilization of primary care, more visits to the ED, and more hospitalizations).
- We often speak about access issues when talking about mental health problems. But it’s important to recognize the full needs of those with major mental illness – yes, there are issues in terms of access to mental health services, but physical health needs must be considered and addressed too.
- The paper asks a good question and finds the answer that we suspect it would. But the contribution here is the actual data. Drawing on databases that cover millions of Ontarians, the authors are able to demonstrate the difference between the diabetic care of those with and without schizophrenia.
- Once again, Dr. Paul Kurdyak pushes us.
Lessons from Sweden
“Guest Post: Ali Damji (Canada) – Snapshots of Patient Co-Produced Care”
Ali Damji
Co-learning with Qulturum, 5 March 2017
https://qulturum.wordpress.com/2017/03/05/guest-post-ali-damji-canada-snapshots-of-patient-led-care/

Time really flies when you’re having fun!
This is my second reflection, from when I participated in a Study Visit with a team from Singapore Institute for Mental Health (all of us pictured above). It was co-learning at its finest, where I not learned about quality improvement and healthcare in Jonkoping, but also a great deal about Singapore too!
One of the main reasons that I traveled to Jonkoping was to learn about patients as partners, and patient-led care. This blog post will focus on a few encounters where patients co-produced better care that I witnessed firsthand.
 Ali Damji
Ali Damji
In this essay, University of Toronto medical student Ali Damji describes his experience learning about health care in Sweden.
He notes several aspects of the Swedish health care system that are different from the Canadian system.
- Patients are invited to attend and participate in ward rounds.
- Self-management includes self-dialysis.
- Hospital staff wear a similar uniform as it’s been shown to reduce infection rates. (Ali is wearing this uniform in the picture above).
He discusses at some length the inclusion of “Esther” in discussions.
In Jonkoping, one of the key ingredients to their successes is a flipped perspective when thinking about quality improvement and change. Rather than thinking about, ‘What’s best for the system? Or what’s best for me, the provider?’, the question always is, ‘What is best for Esther?’ Esther is a hypothetical patient that many of us in healthcare are familiar with. She is a person with a life beyond the walls of the institution, not purely a patient. She is elderly and frail. She has complex health needs. She lives alone. If she lacks effective primary care or transitions from the hospital back to home without support, she does not do well. She’s called a ‘frequent flyer’. But what about the other elements of her life? What drives her? What motivates her? And most importantly, what matters to her? And how is her problem, our problem (not long term care’s problem or the hospital’s problem – our collective problem!)? How can connections be developed and the system be built so it can respond to the things that matter most to her, beyond simply her medical needs?
Ali notes that Esther is considered at various levels of decision-making, even with program funding
A few thoughts:
- This is a fun and lively blog. It doesn’t directly tie into psychiatric care, but does tie into patient care.
- There are a couple of other blogs in the series and the observations on Swedish health care are worth reading. So often we look at other health care systems through the narrow prism of funding; this blog is broader in perspective.
- Ali has just been accepted into the University of Toronto’s Family Medicine program. Congratulations. We look forward to reading more health-care insights from him in the coming years.
- You can find his other Swedish blogs here:
https://qulturum.wordpress.com/author/alidamjiblog/
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments