From the Editor
Anxiety disorders are common, and often disabling to our patients. While treatments have improved, there is unmet need – and the desire to find new, scalable interventions. Increasingly, our patients look to different types of treatments, like yoga. But is trendy effective? Is yoga the not-so-new intervention we need?
Dr. Naomi M. Simon (of New York University) and her co-authors look at the treatment of generalized anxiety disorder with a sophisticated study. They compare yoga and cognitive behavioral therapy (CBT) against a psychological control condition, and against each other. So how do the treatments compare? “Kundalini yoga can reduce anxiety for adults with generalized anxiety disorder, but study results support CBT remaining first-line treatment.” We look at the big study and its big implications.

What have we learned about COVID-19 and mental health? In the second selection, we consider a new editorial from The Lancet Psychiatry. Mulling the state of the literature after almost a year of the pandemic, they write: “The good news is that by October, 2020, mental health was top of the charts in terms of published papers and preprints on the effects of COVID-19. The bad news is that the quantity of papers is not matched by quality.”
And in our final selection, we consider an essay by Rob Whitley (of McGill University). He notes that 27% of Canadians had used cannabis in the last year, about half of them for medical reasons. He worries about the stigma around medical cannabis and champions more public education. “This can help create a climate of acceptance and inclusion for the growing number of Canadians with mental illness who use cannabis to improve their well-being.”
On another note: in a past Reading, we featured an essay by Toronto filmmaker Rebeccah Love who wrote about her mental illness. Her new film, “Parlour Love,” has its premiere this Saturday at 7 pm EST through Zoom. In this short, powerful film, she draws from her own experiences of bipolar mania and psychosis, and paints a portrait of a woman in crisis. RSVP – palmpremiere@gmail.com.
DG
Selection 1: “Efficacy of Yoga vs Cognitive Behavioral Therapy vs Stress Education for the Treatment of Generalized Anxiety Disorder: A Randomized Clinical Trial”
Naomi M. Simon, Stefan G. Hofmann, David Rosenfield, et al.
JAMA Psychiatry, January 2021
![]()
Generalized anxiety disorder (GAD) is a common condition associated with significant distress and impairment,yet only approximately half of affected individuals seek care, with only one-third seen in specialty mental health settings, suggesting a substantial treatment gap.Although cognitive behavioral therapy (CBT) is an effective first-line evidence-based psychotherapy for GAD, many patients do not receive CBT because of cost, stigma, or logistical reasons. Similarly, pharmacotherapy may not be accessible, tolerated, or fully effective.Patients increasingly seek alternative interventions, such as yoga, often outside the medical system.
Yoga offers a popular and promising but underresearched intervention for anxiety. Traditional forms of yoga incorporate physical postures and exercises, breath regulation, relaxation, and meditation and mindfulness practice. The practice of yoga for health purposes has increased markedly, with 14.3% of the US population practicing in 2017. Although mindfulness-based approaches have efficacy for anxiety disorders, including GAD, the efficacy of yoga is less clear. Meta-analyses of yoga for anxiety have yielded inconclusive results, finding that additional rigorous investigations of yoga’s efficacy for anxiety disorders (including GAD) are needed…
The primary aim of the current randomized clinical trial (RCT) was to examine the short-term efficacy of KY compared with (1) a previously validated and standardized control condition, stress management education (stress education [SE]) and (2) a first-line psychotherapy, CBT for GAD…
So begins a paper by Simon et al.
- Recruiting participants from two specialty academic centres, they did a “randomized, 3-arm, controlled, single-blind (masked independent raters) clinical trial” to evaluate the efficacy of 12 weeks of Kundalini yoga (KY), CBT, and stress education (SE).
- Inclusion criteria included: diagnosis of generalized anxiety disorder based on a structured interview.
- Exclusion criteria included: PTSD, substance, bipolar.
- Participants were recruited from December 1, 2013 to October 25, 2019.
- The interventions: the yoga protocol included physical postures and exercises, breathing techniques, relaxation exercises, meditation and mindfulness practices, and yoga theory; the cognitive behavioral therapy used five core treatment modules (psychoeducation, cognitive restructuring, progressive muscle relaxation, worry exposures, and in vivo exposure exercises); stress education included lectures on physiologic, psychological, and medical effects of stress and the importance of exercise and diet.
- The primary outcome was treatment response, as measured by a CGI scale.
- Primary analyses included superiority testing of Kundalini yoga and CBT vs stress education and noninferiority testing of Kundalini yoga vs CBT.
Here’s what they found:
- 226 were selected. They were, on average, in their 30s (mean age = 33.4) and female (69.9%).
- They were randomized to yoga (n=93), CBT (n=90) and stress education (n=43).
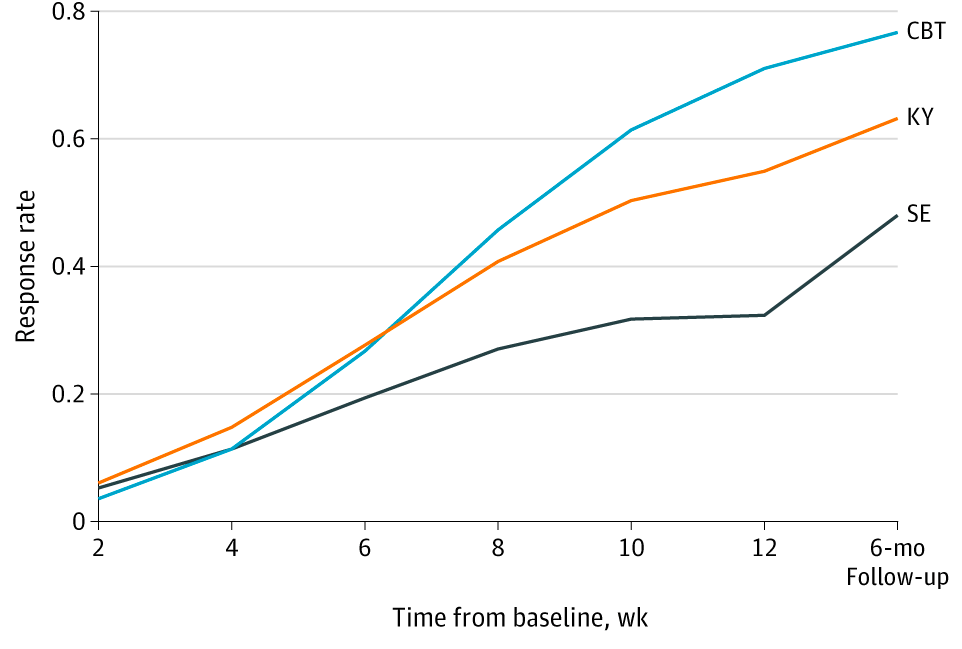
- Response rates at the posttreatment assessment were higher in the KY (54.2%) vs the SE group (33.0%) (number needed to treat, 4.59). Response rates were also higher in the CBT (70.8%) vs the SE group (33.0%) (number needed to treat, 2.62).
- “All 3 treatments were well tolerated with no related serious adverse events”
- “This RCT of adults with GAD found that group CBT was more effective than a previously validated active control condition (SE) matched for time and instructor contact. The CBT RR was 70.8% compared with 33.0% for SE. As hypothesized, KY also had a greater short-term RR (54.2%) than SE, supporting the anxiolytic effects of yoga for patients with a primary diagnosis of GAD. In contrast to our hypotheses, however, we failed to find KY noninferior to CBT, although superiority analyses did not conclusively indicate greater short-term CBT efficacy.”
A few thoughts:
- This is an excellent study.
- The results seem quite reasonable: yoga bested stress education but not CBT. Isn’t that what we expected? CBT has its critics – but it also has its robust evidence in the literature.
- Limitations? The authors note several, including that the yoga and CBT provided in an academic setting may be different from those found in a community setting.
- In an interview for JAMA Psychiatry, the first author spoke about the choice of Kundalini yoga, which includes mindfulness techniques. She felt that that the mindfulness was very important. The full interview with Dr. John Torous (of Harvard University) can be found here:
https://edhub.ama-assn.org/jn-learning/audio-player/18532707.
- So how should we view yoga? It’s growing in popularity, and increasingly the focus on research. For enthusiasts, this paper may be something of a disappointment. But yoga does bestow an advantage over stress education (which seems more robust than the usual care found in many clinics). While yoga can’t be viewed as the only treatment, this paper bolsters the argument that it should be considered in treatment recommendations to patients. And for those patients with anxiety who hesitate on CBT and medications, yoga – at least the Kundalini type – has evidence.
The full paper can be found here:
https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2769486
Selection 2: “COVID-19 and mental health”
The Lancet Psychiatry, February 2021
![]()
While the effects of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) on the nervous system remain unclear, there is no doubt that the COVID-19 pandemic is bad for mental health. To alleviate the impact of both the virus and the measures taken to control its spread, we need high quality information about their immediate and long-term effects, and which countermeasures are most effective. The good news is that by October, 2020, mental health was top of the charts in terms of published papers and preprints on the effects of COVID-19. The bad news is that the quantity of papers is not matched by quality. In March, 2020, Holmes and colleagues outlined the priorities for mental health research during the pandemic. How much have we learned since then?
So begins a short editorial from The Lancet Psychiatry.
The authors argue that many things remain unclear with the pandemic: “For people with mental illness, database studies so far have produced contradictory findings: in South Korea, a history of mental illness was not associated with increased likelihood of testing positive for SARS-CoV-2, but patients with a history of severe mental illness had a slightly higher risk for severe clinical outcomes of COVID-19 than patients without such a history. In the USA, a recent diagnosis of a mental disorder was associated with an increased risk for infection, which was exacerbated among African Americans and women, and a higher frequency of some adverse outcomes of the infection.”
The editorialists note that many questions need to be answered: “how best to deliver mental health services for vulnerable groups, outreach methods to support those at risk of domestic abuse, how media consumption about COVID-19 influences mental health, and how to promote adherence to behavioural advice about COVID-19 while enabling mental wellbeing and minimising distress.”
A few thoughts:
- This is a strong editorial.
- Ultimately, they call for more research.
- The comment about the quality of research resonates. As noted in a past Reading, many studies confuse symptoms and disorders, leaving the impression of far-reaching mental health problems that may not be anchored in reality.
The editorial can be found here:
https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366(21)00005-5/fulltext
Selection 3: “Destigmatize cannabis use for mental health”
Rob Whitley
Vancouver Sun, 14 January 2021
![]()
Health Canada just released the results of its 2020 Canadian Cannabis Survey, noting that a whopping 27 per cent of Canadians had used cannabis in the last year. Approximately half of those surveyed stated that they used cannabis for medical purposes, with rates of usage particularly high among people reporting poor or fair mental health.
These findings overlap with the existing research which indicates that a substantial number of people with mental illness use cannabis therapeutically to manage symptoms such as anxiety, sleep issues and chronic pain. Such medicinal usage can reduce suffering, as cannabis contains analgesic properties that are generally effective and safe when used in moderation.
In sum, around one in seven Canadians are using cannabis for medicinal purposes, many of whom have mental illness, and this can have a positive effect on their quality of life and overall well-being.
So begins a short essay by Whitley.
He notes that cannabis has been legal for over two years, yet: “there are still many stereotypes and stigmas surrounding people who use medicinal cannabis, which can lead to discrimination and exclusion. For example, one study from the University of British Columbia found that medicinal cannabis users were frequently labelled as irresponsible, unreliable and unsavoury ‘potheads’ by a variety of people including family, friends and even healthcare providers.”
Whitley argues that some turn to cannabis because other treatments failed. “One veteran told the [Senate] committee that ‘medical cannabis saved his life and…improved his quality of life by exponential dimensions.’”
“In short, the stigmas and stereotypes surrounding cannabis users are obscuring the reality that many people from many walks of life are now using cannabis for beneficial health purposes.”
He notes several efforts to educate the public, including a project that will produce educational documentaries; he is involved in it.
A couple of thoughts:
- Whitley argues his points well.
- As health care providers, should we be comfortable with efforts to destimatize the use of cannabis when there is so little evidence in the literature favouring its use for conditions like depression and anxiety? Should our role be to provide better balance to the billion-dollar industry promoting cannabis as a panacea? Or is Whitley right – our patients find cannabis helpful, and we should help reduce societal judgment?
The full essay can be found here:
https://vancouversun.com/opinion/time-to-destigmatize-cannabis-use-for-mental-health
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments