From the Editor
Almost two decades ago, I was invited to a conference. The keynote speaker was Michael Wilson, the former federal Minister of Finance, who died earlier this month. I remember two things about this presentation: first, the audience was perfectly still – as Wilson spoke about his son’s suicide, no one shuffled her papers or chatted with his neighbour; second, I remember thinking how unusual this presentation was: he spoke about suicide at a time when suicide wasn’t discussed.
This week, we look at three selections, including an interview in which Wilson discusses his decision to speak out.
We also consider two other pieces: a new study on psychotherapy for inpatients with depression and an essay considering whether patients are experts.
 Michael Wilson
Michael Wilson
Enjoy.
And I hope you will take a few minutes to complete our survey, aimed at improving the Readings.
https://www.surveymonkey.com/r/GP5XXMB
DG
Selection 1: “Efficacy of inpatient psychotherapy for major depressive disorder: a meta‐analysis of controlled trials”
C. Schefft, A. Guhn, E.‐L. Brakemeier, P. Sterzer, S. Köhler
Acta Psychiatrica Scandinavica, 5 December 2018 Online First

Major depressive disorders (MDD) are the leading cause of disability worldwide affecting over 300 million people. The lifetime risk for depression is in the range of 16–20% with rates of chronicity as high as 30%. MDD ranks fifth among the causes of years lived with disability. Many treatment strategies have been proven to be effective in the treatment of MDD, including various classes of antidepressants and various types of psychotherapeutic interventions. The combination of pharmacotherapy and psychotherapy proved to be superior to both pharmacological and psychological treatment alone in moderate to severe MDD. Therefore, several guidelines recommend the combination of pharmacotherapy and psychotherapy for patients with a moderate or severe depressive episode.
However, most of the studies to which guidelines refer were performed in outpatients. Of note, inpatient psychotherapy remains an important treatment option for patients with severe and chronic depression, especially if they cannot safely stay in their own environment or appear as treatment‐resistant to outpatient interventions. Indeed, patients with treatment‐resistant depression (TRD) demonstrate high rates of suicidality and psychiatric comorbidity. At least in some countries, inpatient treatment is applied frequently for this highly burdened patient population.
So begins a paper by Charité-Universitätsmedizin Berlin’s Cora Schefft et al. considering inpatient psychotherapy. They did a meta-analysis that drew from various databases (including MEDLINE and PsycINFO), with inclusion criteria of adults having a diagnosis of depression, and having some type of psychological intervention (group or individual) compared against control. They found 14 studies involving just over a thousand patients.
The therapy made a difference:
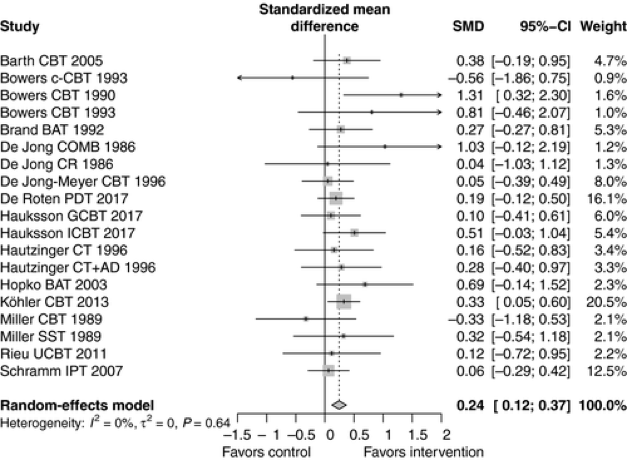
The authors also looked at subgroups, including accounting for intensity of therapy.
The result? “Confirming the results of this previous study, our present meta-analysis suggests asmall but significant effect of inpatient psychotherapy on depression severity.” The number needed to treat was 7.4. The authors also found that the result was stable over 12 months.There are many challenges to providing psychotherapy on an inpatient basis (think length of stay burden of illness, etc.). Still the result is clear, and pushes us to see inpatient care as being more than medications and the safety of hospitalization.
Criticisms of the work? This is a good study, though I note that the meta-analysis drew from studies over many years – going back to 1986. Inpatient care has changed over these past decades, with the length of stay tumbling. An eyeball of the results suggests that excluding older studies would still have yielded a positive result.
The full paper can be found here:
https://onlinelibrary.wiley.com/doi/10.1111/acps.12995
Selection 2: “From the archives: The late Michael Wilson on his son’s suicide and mental-health care in Canada”
André Picard
The Globe and Mail, 11 February 2019
![]()
‘I started searching for him. By pure accident, I found him wandering the streets. It was the middle of December, it was cold, and he was in slippers,’ Mr. Wilson says in a hushed voice. ‘He was hallucinating, imagining things. He was clearly a very sick young man. Cam needed help.’
Michael Wilson served in many roles – ambassador, Minister of Finance, Bay Street executive – but the article talks about his decision to speak out about his son’s suicide.
Wilson died earlier this month, and many tributes have been written. This article from The Globe draws from an interview done nearly twenty years ago. It was then that Wilson chose to champion the fundraising campaign of the Centre for Addiction and Mental Health (CAMH). Wilson could have simply endorsed the effort, but instead he made it personal. He spoke about the decision:
‘There are not many things in life as hard as coming to grips with the fact that your child is suffering from mental illness,’ Mr. Wilson says. He grew up believing that depression and addiction were signs of moral weakness, not diseases. He is also of an era when you didn’t talk of such things.
But convinced that the mental-illness stigma contributed to his son’s demise, he has vowed to change that reality.
As I mentioned at the opening of this Reading, the decision was highly unusual.
So was the fundraising campaign. When Wilson leant his name to the effort, consultants had warned CAMH that their fundraising goal was overly ambitious for a mental health cause. For the record, CAMH made the goal; the last campaign raised over $200 million. Times have changed. People like Wilson helped change them.
The Globe piece can be found here:
Many have paid tribute to Michael Wilson and his work. The University of Toronto put together a compilation, including comments from prime ministers, cabinet ministers, and others, which can be found here:
For the record, CAMH President and CEO Catherine Zahn seems to have said it all in just a sentence: “A Canada without Michael Wilson is a smaller place.”
Selection 3: “The risks of equating ‘lived experience’ with patient expertise”
Frank Gavin
healthydebate, 13 February 2019
![]()
Does being a patient make you an expert? The Canadian Institutes of Health Research (CIHR), the country’s largest funder of health research, certainly seems to think so. Eight times in the patient engagement framework for its Strategy for Patient-Oriented Research (in which patients are partners in all phases of the research process), the CIHR attaches the word ‘expert’ or ‘expertise’ to patients.
There appears to be a hedge, however. In one statement, patients are said to ‘bring the perspective as ‘experts’ from their unique experience and knowledge.’ Why the quotation marks around “experts,” which to me seem to qualify or even question the view that patients are actual experts? If it were simply a statement of fact, the quotation marks would not be needed.
Most of the time when patients are called—or call themselves—experts, there are no quotation marks, no hedging. That patients, especially those living with chronic conditions, are experts is, for many, not just a fact but a conviction. It’s not hard to understand why this is so. Health care and health research are full of experts whose status is signalled by white coats, titles, lots of letters after their names, and much deference directed their way. There are specialists and sub-specialists as well as fellows and post-docs—and not just among physicians. It is a very hierarchical world in which expertise is the coin of the realm.
Writing for healthydebate, Gavin – who is chair of the Citizen Engagement Council of CHILD-BRIGHT, a CIHR SPOR national research network focused on children with brain-based disabilities and their families – writes about patients as experts.
He finds problems with the concept.
One difficulty is understanding what exactly patients are expert about. Experts, whether they are medical specialists, computer scientists, or historians, have well-defined and usually quite narrow areas of expertise. To achieve expert status they have had to demonstrate their knowledge and skills in relation to clear standards, and have had that knowledge and those skills rigourously assessed and, one hopes, re-assessed. Never infallible, their opinions carry extra weight within their fields but not outside them.
He notes his own experience as a person with illness: “While this made me more knowledgeable than most about Guillain-Barre, the only thing I know very well about the condition is my experience of it.”
He notes other problems with the concept of patients as experts:
- “Another problem is the anxiety that the expectation of expertise sometimes imposes.”
- “The final problem resulting from of the idea that patients are experts is that it may not do justice to—and it may even obscure—the deep experiential knowledge nearly all of them possess.”
To be clear, Gavin sees a role for patients being involved. He concludes: “We don’t have to be experts to be equal.”
In an age of co-design, this article asks thoughtful questions.
The piece – which is highly readable – can be found here: https://healthydebate.ca/opinions/patients-as-experts
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
February 28, 2019 at 1:18 pm
Many thanks for letting us know about Frank Gavin’s thoughtful and sensible examination of issues related to seeing patients as experts.
The idea of empowering some patients as experts is very problematic when it comes to mental illnesses. People with more mild conditions are told they are experts based on their own experiences. The Mental Health Commission of Canada has built an expanding infrastructure based on this notion in their guidelines for training and supervising peer support workers. Their guidelines don’t require or even suggest that peer training programs teach anything about mental illnesses; in fact, many peers hold the fashionable opinion that mental illnesses aren’t real illnesses. This is becoming a workforce that can undermine medically necessary treatments.
I discuss these problems in these two articles:
https://www.huffingtonpost.ca/susan-inman/peer-mental-health-workers_b_9009252.html
https://thetyee.ca/Opinion/2018/10/25/New-Standards-Fail-Mental-Illnesses/