From the Editor
Another tragedy, another headline.
And there have been too many. The stories differ, but there is a common thread: mental illness and a crisis, a 911 call, death. Can we do better?
In the first selection, we consider a new essay by Dr. Sally Satel (of Yale University). Dr. Satel, a psychiatrist, notes recent tragic outcomes with mental health crises. “Nationwide, a person with a psychotic illness is 16 times more likely to be killed during a police encounter than a person without such a condition.” She wonders about an alternative to police responses.

In the second selection, we look at apps and college students. In a Psychiatric Services paper, Jennifer Melcher and John Torous (of Harvard Medical School) review the recommendations of mental health apps of several university counselling programs. They conclude: “the findings indicated that many counseling centers are suggesting apps that are inaccessible, outdated, potentially dangerous, and without research backing.”
Finally, in our third selection, we consider The New York Times obituary for D.J. Jaffe – the title is a good summary of his life: “Ad Man Turned Mental Health Crusader.” Jaffe, whose sister-in-law has major mental illness, was a strong advocate of various mental health causes, with his influence felt on state and national legislation.
DG
Selection 1: “Rethink Crisis Response”
Sally Satel
Reason, October 2020
![]()
‘Please just send one police car, please don’t have your weapons drawn, please take him to the hospital.’ These are the words that many families with a mentally ill loved one have learned to say when crisis strikes. Sabah Muhammad and her siblings have spoken them several times since 2007, the year her brother was diagnosed with paranoid schizophrenia. He had been a standout student and star running back at his high school near Atlanta, but everything changed around his 18th birthday. ‘He would become catatonic, barely moving, just staring into space,’ Sabah explains. ‘Sometimes he locked himself in his room for weeks, refusing food, except to come out of his room at 3 a.m. to make toast that he blackened to carbon ‘to get the poison out.’
Mute and malnourished, he would not allow family to take him to a psychiatrist – but he desperately needed help. The only option in the Muhammads’ Atlanta jurisdiction was a 911 call to report a psychiatric emergency, which tended to bring the police, multiple squad cars with lights flashing, and the ominous specter of armed agents encountering a young black man in a delusional state. So Sabah and her family would call the police, and pray.
The data justify their dread. Between 25 and 50 percent of all people killed annually by police are in the midst of a mental health crisis when they’re slain, according to a report by the Treatment Advocacy Center (TAC), a Virginia-based nonprofit dedicated to improving treatment for people with serious mental illnesses.
So begins an essay by Dr. Satel.
She notes several tragedies. She then wonders about the nature of police culture. She quotes New York Police Department Assistant Chief Matthew Pontillo: “Cop culture has always been, ‘We’re the people who respond to a crisis, jump out of the car, and take immediate action…’”
What about training? Many police departments have mandated Crisis Intervention Team training, but there is scant evidence:
- “A 2014 meta-analysis revealed no differences in arrests or use of force between officers who were and who were not trained…”
- “A 2019 review of research found rampant variability within training programs; and another analysis, from the Police Executive Research Forum, found that participants sometimes spent as little as eight hours in training.”
- “In New York City, where half of the police force has undergone CIT training since 2015, 16 people with mental illness have been killed in encounters with law enforcement since the training began, exceeding the number killed in the five years prior to initiation of the program.”
Dr. Satel wonders about alternatives. She focuses on CAHOOTS:
“One of the nation’s longest-running examples of this [alternative] is CAHOOTS (Crisis Assistance Helping Out On The Streets). It was created 31 years ago as part of an outreach program of the White Bird Clinic in Eugene, Oregon – once a countercultural medical clinic founded in 1970 as a refuge for hippies on LSD trips and other drug-taking youth. Calls for help are routed to staff 24/7 by the local 911 dispatcher. A medic and a mental health professional respond as a team to incidents such as altercations, overdoses, and welfare checks. They wear jeans and hoodies and arrive in a white van stocked with supplies like socks, soap, water, and gloves. Should a situation spin out of control, they call for CIT-trained police back-up, though last year only 150 out of 24,000 field calls required back-up. People who need further attention are taken to a crisis care facility operated by the mental health department – no trips to jail or to overflowing emergency rooms.”
A few thoughts:
- This is an excellent essay.
- The description of CAHOOTS is compelling. Some have argued against a non-police model because of the potential for danger. Yet well under 1% of field calls require back-up.
- A word of caution. It’s difficult to implement a program that has been created elsewhere, responding to different circumstances. Canadian jurisdictions would ultimately need a “made in Canada” solution. Still, looking abroad for ideas is reasonable, and Dr. Satel’s essay is thus timely and relevant.
The full essay can be found here:
https://reason.com/2020/09/13/rethink-crisis-response/
Selection 2: “Smartphone Apps for College Mental Health: A Concern for Privacy and Quality of Current Offerings”
Jennifer Melcher and John Torous
Psychiatric Services, 15 July 2020 Online First

Colleges continue to see a dramatic surge in mental health needs among students in the past few years. The percentage of students with diagnosed mental health conditions increased from 22% to 36% between 2007 to 2017, although there has not been a concomitant increase in services offered. The 2019 American College Health Association National College Health Assessment found that in the past year, 13% of college students had seriously considered suicide and 2% of college students had attempted suicide. Students are increasingly visiting college counseling centers for help, and the centers are expected to absorb the expanding load. Between the beginning of the 2009 academic year and the end of the 2015 academic year, counseling center utilization by college students increased on average by 30%-40% per school while the enrollment for these schools increased by only 5%. That is, a greater percentage of college students are seeking help at counseling centers than in the past. Previous research suggests that one reason for the increased use of college counseling centers is a reduction in stigma associated with mental illness and mental health treatment.
So begins a paper by Melcher and Dr. Torous.
Here’s what they did:
- Drawing on national college rankings, they selected counseling centres of sixty colleges and searched their web sites for “for any reference to self-help apps or apps as resources for students.”
- The features of apps were then considered – including “last update, privacy policy, and whether any research had been published in peer-reviewed journals.”
Here’s what they found:
- “Results from this analysis indicated that 26 (43%) of the 60 schools suggested apps on their Web site.”
- “A total of 218 unique apps were suggested across the schools. Counseling centers suggested between 1 and 85 apps…”
- The apps represented 8 categories: health and fitness, lifestyle, medical, productivity, games, education, utilities, and entertainment.
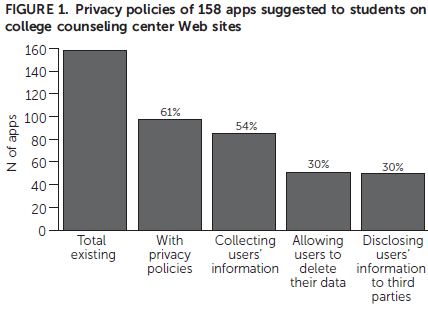
- Availability. “28% were no longer available for download.”
- Updates. “Of the 158 remaining apps, only 44% had been updated in the past 6 months.”
- Privacy. “39% had no privacy policy. Of the 97 existing apps with privacy policies, 88% collected user’s data and 49% shared users’ data with third parties.”
- Evidence. “Efficacy studies had been published in peer-reviewed journals for only 16% of existing apps.”
- This is a good study.
- Apps are part of the way we live, work, and receive care – including mental health care. It’s striking how many schools recommend apps. This is an American paper, and the colleges were all in the United States. Would the findings be any different if the authors had considered Canadian schools?
- The attraction of apps is obvious. As the authors note: “Digital solutions are relatively cheap and easy to implement across an entire campus. These solutions can decrease the number of students who need to seek out in-person counseling, and they can also be used as an addition to care.”
- “With 26 schools suggesting a total of 218 unique apps, students are left to sort through all the suggested apps to find one for themselves without clinical input.” Ouch. And there are problems with the recommendations, which include many apps that can’t even be downloaded. Ouch.
- Digital privacy has come up in past Readings. Again, there is cause for concern. The data here suggests that many apps share data with third parties. Ouch.
The full paper can be found here:
https://ps.psychiatryonline.org/doi/10.1176/appi.ps.202000098
Selection 3: “DJ Jaffe, Ad Man Turned Mental Health Crusader, Dies at 65”
The New York Times, 16 September 2020

While DJ Jaffe was working as an advertising executive on Madison Avenue, he and his wife became the caretakers of his wife’s half sister, who had moved from Milwaukee as a troubled teenager to live with them in their Manhattan apartment. Before long she became catatonic. She was later found to have schizophrenia and bipolar disorder.
The experience plunged Mr. Jaffe, who died on Aug. 23 at 65, into the world of mental health, which he soon came to see as dysfunctional.
It also turned him into a crusader.
The obituary notes his primary cause: “Kendra’s Law, a controversial measure passed in New York State in 1999 that authorized the courts to mandate outpatient psychiatric treatment for people who might pose a danger to themselves or others. If they fail to comply, they can be seized by police and hospitalized for a three-day lockup period.”
Jaffe was in advertising, where he enjoyed success:
“Mr. Jaffe was recruited by Coopers & Lybrand, the accounting firm, which later became PricewaterhouseCoopers, and he moved to Chicago. Only then, by his account, did he realize that he hated accounting. After putting out the word that he was available, he was recruited by an advertising agency and moved back to New York.” He worked on several big accounts, including Coke.
But his passion was advocacy. The article notes that he wrote books as well as opinion pieces, espousing what he called “treatment before tragedy.”
He championed assisted outpatient therapy – what we would know as community treatment orders (CTOs) in Canada.
“Critics argued that the law impinged on the civil liberties of these patients. And by 2005, racial disparities were reported in its use, with Black people five times as likely as white people to be subjected to it. But it was also hailed as reducing homelessness, suicide attempts, hospitalizations and incarcerations.”
A few thoughts:
- It’s rare for anyone in mental health to be given an obituary in The New York Times. I can’t recall ever reading such an article for an advocate whose family was touched by mental health problems.
- Jaffe is one of several advocates for Kendra’s Law, which led to legislation across the vast majority of the United States.
- CTOs are controversial, and have been criticized by patients and advocacy groups. But if the goal is to reduce bad outcomes like homelessness and hospitalizations, are CTOs that controversial?
- The NYT article doesn’t talk about his criticism of many mental health programs, including ThriveNYC. Jaffe believed that health care funding should help those with severe illness, not offer mental wellness initiatives.
The full obituary can be found here:
https://www.nytimes.com/2020/09/16/nyregion/dj-jaffe-dead.html
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
October 4, 2020 at 8:36 pm
Thank you so much for calling attention to the extraordinary work of DJ Jaffe.
I think his book, Insane Consequences: How the Mental Health Industry Fails the Mentally Ill, has tremendous value for Canadians, not just Americans, who want to understand why and how mental health services don’t meet the needs of people with the most severe mental illnesses.
I’m one of the many fortunate family members who DJ mentored in recent years. He helped us understand the chaos we witness and actions we can take to try to address the problems we see. In my last article, I look at how disability rights organizations fail people with schizophrenia while, at the same time, they are assumed to represent them:
https://medium.com/@suinman/disability-rights-groups-should-accept-schizophrenia-9b1220c81f2a