From the Editor
Patients with depression benefit from psychotherapy. But do those effects last?
The question isn’t new, but long-term effects haven’t been well studied. An impressive new World Psychiatry study by Pim Cuijpers (of Vrije Universiteit Amsterdam) and his co-authors brings needed data to the discussion. They did a meta-analysis of 191 RCTs with 209 comparisons between treatment and control groups, involving 33 691 participants. “We conclude that psychotherapies have moderate to large effects at 3 months after randomization, which slowly decrease during the next 9 months to a moderate level, and remain stably moderate for several years.” We consider the paper and its implications.

In the second selection, from The American Journal of Psychotherapy, Michelle Geiss (of Southern Illinois University) and her co-authors analyzed a canine-assisted intervention (CAI) on an inpatient unit, drawing on semi-structured interviews with 17 psychiatric nursing staff members. “CAI was perceived by staff as a valuable complementary therapy in the inpatient psychiatric setting, offering emotional, social, and therapeutic benefits for both patients and staff.”
And in the third selection, psychologist Harvey Lieberman reflects on psychotherapy in an essay for The New York Times. As a therapist, he wonders whether too many people seek therapy. “For some people, therapy can help in ways nothing else can. But many will find that the best forms of understanding and emotional support flow from informal networks of relatives, neighbors and friends, not the health care system.”
Note: there will be no Reading next week.
DG
Selection 1: “Long-term effects of psychotherapies for depression: an advanced meta-analysis”
Pim Cuijpers, Clara Miguel, Esra Kaya Aglio, et al.
World Psychiatry, June 2026
It is well-established that psychotherapies are effective in the treatment of depression… It is unclear, however, what the effects of psychotherapies are in the longer term. A previous network meta-analysis found that psychotherapies still have significant effects at one-year follow-up, and in two other network meta-analyses it was found that the effects of psychotherapies are superior to those of pharmacotherapy at one-year follow-up. These studies built on earlier meta-analyses showing that psychotherapies have significant effects at 6-month and longer follow-up. A few other meta-analyses have examined the long-term outcomes of Internet-based interventions for depression and indeed found positive effects at follow-up. However, the number of studies with follow-up data at one year or longer was very limited.
The small number of randomized trials with long-term follow-up is a problem in all previous meta-analyses examining long-term outcomes of psychotherapies for depression. The most extensive meta-analysis included 96 trials, but few of these had a follow-up period of more than one year. Furthermore, in those meta-analyses, all follow-up outcomes were clustered into time categories that were examined in separate analyses. More advanced analyses in which all time points from all studies are modelled simultaneously in one analysis have not yet been conducted in this field. Such analyses also make it possible to examine the trajectory of treatment effects over time, rather than only assessing whether the effects remain significant at specific time points.
So begins a paper by Cuijpers et al.
Here’s what they did:
- They conducted “a comprehensive meta-analysis examining the long-term effects of psychotherapies for depression compared with control conditions.”
- They searched four major databases (including PubMed) up to May 2025.
- They included randomized controlled trials “comparing psychotherapies for adult depression with control conditions (care-as-usual, waitlist, or other) that reported outcomes at six months after randomization or later.” Eligible studies included adults with depression diagnosed by structured interviews or validated symptom scales; studies involving youth and inpatients were excluded.
- Two independent reviewers screened the studies, extracted data, and assessed study quality using the Cochrane Risk of Bias 2 tool.
- The main outcome: the standardized mean difference (SMD) between the treatment and the control condition. They also examined response rates in the treatment and control groups and the relevant risk ratio (RR).
- They evaluated the effectiveness of psychotherapies over time using “a multivariate pooling model with cubic regression splines to allow for potentially non-linear interactions.”
Here’s what they found:
- They included 191 RCTs with 209 comparisons between treatment and control groups, involving 33,691 participants – 17 715 in the treatment groups, 15 976 in the control groups. (!!)
- Demographics and therapy. The mean age was 44.5 years. Most participants were female (72.8%). Many were from Europe (43.4%) or North America (29.8%). Half of the comparisons involved CBT (50.7%).
- Follow-ups. The trials encompassed 534 follow-up measurements, of which 52 (9.7%) occurred more than 12 months after randomization.
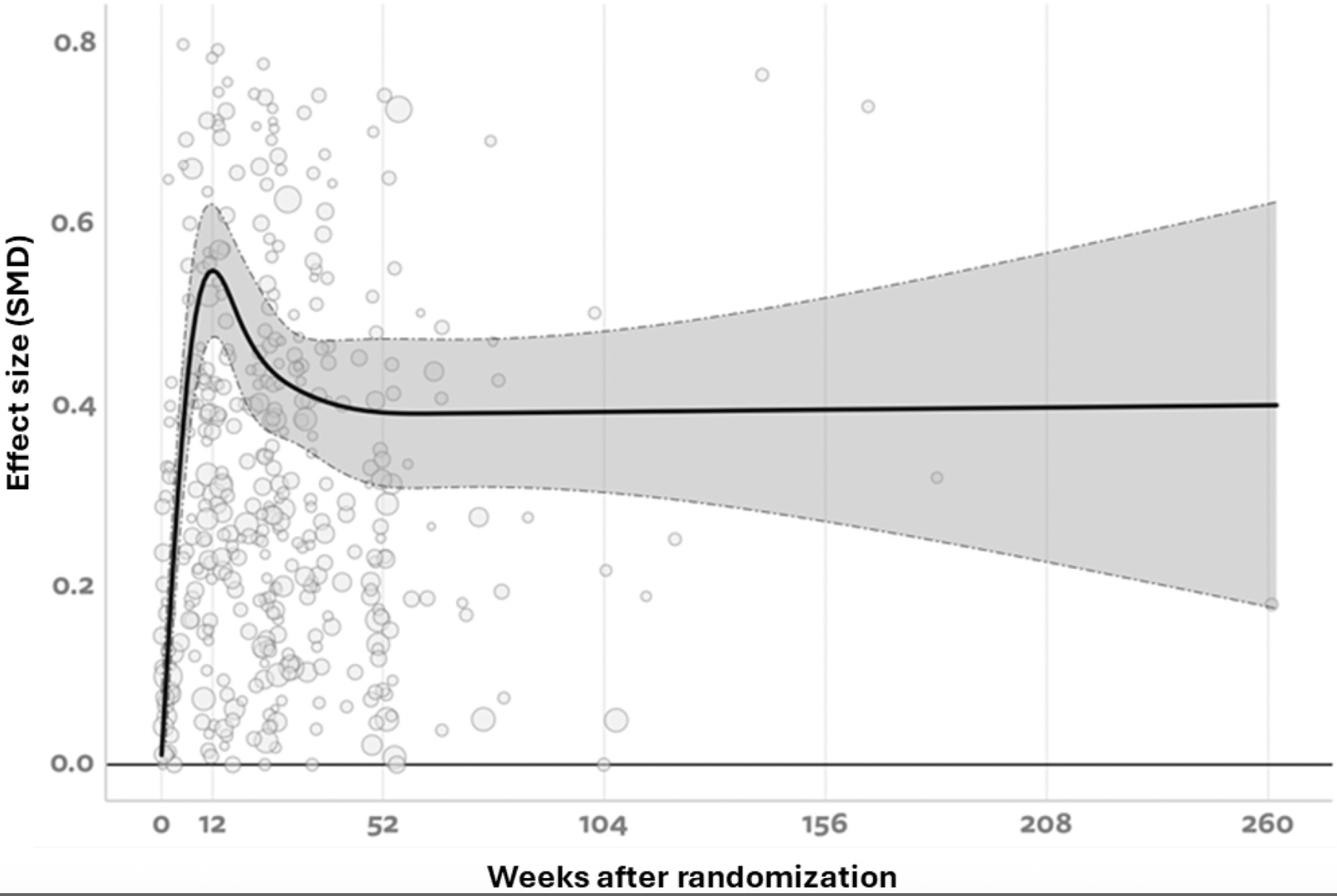
- Effects. “The best fitting restricted cubic spline model for long-term SMDs (5 basis functions) indicated that the SMD increased from baseline to 0.55 at 12 weeks, then gradually decreased to 0.39 at around one-year follow-up, and remained largely stable thereafter.” In other words, the moderate effect observed at one year was maintained. See the graph below.
- Longer term. “The SMD remained statistically significant up to 8.3 years after randomization.” (!)
- Relative risk. “The RR remained significant up to 4.5 years (236 weeks).”
A few thoughts:
1. This is an impressive study with an extraordinary dataset – the authors note that it is “by far the largest meta-analysis of the long-term effects of psychotherapies for depression” – and published in a Very Big Journal.
2. The main findings: “We conclude that psychotherapies have moderate to large effects at 3 months after randomization, which slowly decrease during the next 9 months to a moderate level, and remain stably moderate for several years.”
3. Wow.
4. Was one therapy less effective than others? Though they suggest complexities, they note: “We found that behavioral activation was associated with significantly worse outcomes compared to other psychotherapies.”
5. The authors used complicated statistical analyses. Still, the findings seem right.
6. Like all studies, there are limitations. The authors note several, including: “The number of measurements beyond two years was limited, and many trials had some risk of bias, although we did not find that this risk was associated with the course of the effects over time.”
The full World Psychiatry paper can be found here:
https://onlinelibrary.wiley.com/doi/10.1002/wps.70065
Selection 2: “Canine-Assisted Intervention in the Inpatient Psychiatric Hospital Setting: Staff’s Perception of the Benefits of Pet Therapy”
Michelle Geiss, Lorna Scoggins, Shelby Whaley, et al.
The American Journal of Psychotherapy, 6 April 2026 Online First

Patients with psychiatric disorders are recognized as a highly vulnerable population in the context of inpatient care. Staff often seek new interventions to help patients decompress, increase socialization and engagement, and use coping skills to manage their everyday lives…
Canine-assisted intervention (CAI) is becoming increasingly popular in the hospital setting because of its multiple health benefits. The benefits of human-animal interaction have been associated with lower blood pressure, alleviation of mental stress, and improved autonomic regulation. The use of animals as a therapeutic intervention can create a positive relationship between the animals and patients, providing a calming environment that improves communication of the patients, decreases symptomatology of their mental illness, increases their self-confidence, and improves their overall quality of life… In psychiatric hospital settings, CAI has been found to reduce patients’ fears prior to electroconvulsive therapy and decrease patients’ anxiety and depressive symptoms, pain, and pulse. Several studies have focused on the benefits of CAI among patients with schizophrenia, with patients showing improvements in negative symptoms, increased adherence to treatment, decreased cortisol levels, enhanced socialization, improved well-being, and increased motivation to complete activities of daily living.
So begins a paper by Geiss et al.
Here’s what they did:
- “The authors conducted a 20-minute semi-structured interview with psychiatric nursing staff members who were current employees in an adult inpatient psychiatric unit and who had worked with pet therapy services over the past 4 years.”
- The interviews were conducted at a US hospital.
- Additionally, participants completed a demographic survey that included questions about their age, gender, and ethnicity.
Here’s what they found:
- Demographics. Most participants were female (59%); about half were over the age of 45 years (47%). The vast majority identified as Caucasian/White (94%). Most had worked on the unit for more than 2 years (66%).
- Experiences. “Commonly expressed themes included improved patient mood (18% of responses), excitement (14%), joy (14%), and a sense of reward (14%).”
- Descriptions. “When describing psychological benefits among patients, participants emphasized that CAI fostered emotional uplift (52% of responses), enhanced socialization (12%), and created excitement (8%).”
- Benefits. “The benefits included staff enjoyment (17% of responses), improvement in patients’ mood (13%), and enhanced patient experience (13%).”
- Recommendations. “When asked for recommendations, participants expressed a desire for more frequent therapy sessions (60% of responses).”
A few thoughts:
1. This is an interesting study on a good topic, but with a dataset limited to one hospital and 17 interviews.
2. The main findings: “CAI is viewed by psychiatric nursing staff as a valuable adjunctive intervention that promotes emotional well-being, enhances patient engagement, and contributes to a more positive therapeutic environment in the inpatient psychiatric unit.”
3. Animal therapies are increasingly popular. This paper contributes to the literature – though more work is needed in the area. Still, there is a pattern. “Staff observed that patients who were often withdrawn became more open and communicative when interacting with therapy dogs. This finding mirrors those of Berget et al. indicating that animal-assisted therapy fosters trust, empathy, and a sense of safety – key components in therapeutic relationships within psychiatric settings.”
4. The paper includes details from the program and even a photo of one dog. For the record, Kylo is a good-looking doggie.

The full Psychiatric Services paper can be found here:
https://psychiatryonline.org/doi/10.1176/appi.psychotherapy.20250082
Selection 3: “I’m a Therapist. Not Everyone Should Be in Therapy.”
Harvey Lieberman
The New York Times, 5 July 2026

As a clinical psychologist with over 50 years of experience, I know that therapy can be essential. A person with persistent intrusive thoughts can learn ways to reduce their intensity. Someone in an acute crisis can hear a perspective that helps steady his or her thinking.
But I hear from former patients and colleagues that people are often turning to therapy not because of disordered thoughts, but because of difficult circumstances: loneliness, conflicts at work, financial strain. Therapy seems to have become the default prescription for all forms of unhappiness.
Anyone who simply needs a listener may get something out of therapy. But when every struggle is routed toward a professional, we risk mistaking mental health issues that require treatment for problems of isolation or circumstance.
So begins an essay by Lieberman.
“Unhappiness is often not a disorder, but a structural condition. In 2023, the U.S. surgeon general identified loneliness and social isolation as urgent public health concerns. He pointed to an erosion of everyday social connection as a central cause, yet much of the response has focused on expanding clinical access rather than rebuilding relational life. In 2019, about one in 10 American adults reported receiving counseling or therapy. By 2024, that figure had risen to roughly one in seven.”
He notes the implications for care. “The cracks in the clinical system are beginning to show. In many regions, therapy wait lists stretch for months, and clinicians report burnout. Patients with the most disabling conditions are left competing for the limited time, and those who are primarily seeking friendship and connection may leave feeling disappointed.”
He draws a line with therapy. “Part of the confusion lies in what therapy reliably provides. When it is effective, it often helps with persistent problems that come from within: obsessive thoughts that return no matter how often you try to dismiss them, fears that repeatedly damage relationships, periods of despair that continue even when life circumstances improve. Therapy can be especially useful when people’s habits deepen their suffering, or when painful experiences remain difficult to make sense of alone. But when distress is shaped primarily by situational difficulties or the absence of community, therapy may not be the best fit.”
He provides examples. “Consider a few situational difficulties: child care frustrations, anxiety after relocating to a new place, a family dispute. Sometimes, these problems can affect thinking in ways that therapy can help resolve. But on their own, these issues do not necessarily require clinical intervention. They can be painful without reflecting a disorder.”
“Some people would say that a therapist’s consistent, neutral perspective would help anyone. It’s true that many people benefit from having a place to think and to be heard, and from a therapist’s disciplined attention. But therapy’s tools are limited.” He draws from his own experience. “In my own practice, I helped patients understand their problems in a new light – but those insights could go only so far if their circumstances remained unchanged. Some who came in after a life crisis told me that after a few sessions, they began reconnecting with friends and family, seeking support they had not known how to ask for during the crisis. Looking back, I suspect that restoring those connections often mattered as much as anything we discussed in my office…” He adds: “As the boundary blurs between a disabling disorder and ordinary distress, people may start to view their suffering through a clinical lens. But often, distress functions less as a symptom than as a signal. Feeling anxious does not mean you have an anxiety disorder. It could point to circumstances that are worth changing.”
He sees a path forward. “Before turning to therapy, consider reaching out to someone you trust, volunteering, joining a community activity or reconnecting with a group that once mattered to you. Meaningful relationships rarely develop overnight, but those are all small steps toward deep connections. Sometimes hope arrives before companionship does. If your distress continues to interfere with daily life and relationships, therapy may be the right next step.” He adds: “Rebuilding relationships should not fall entirely on individuals, but also on schools, workplaces and governments.”
He continues: “Many of the institutions that shape social connection – libraries, schools, recreation programs – are organized and supported locally. Government agencies could help communities measure loneliness, identify groups at greater risk and support outreach efforts that connect residents to existing resources. The challenge is often not creating new opportunities for connection, but helping isolated people discover and participate in the ones that already exist.”
A few thoughts:
1. This is a good essay.
2. He makes solid observations.
3. Has therapy’s role grown too large in part because of the medicalization of stress?
4. To play the devil’s advocate: is the problem that many people aren’t sick enough for limited psychotherapy resources – or that there aren’t enough services that are available in the United States?
The full New York Times essay can be found here:
https://www.nytimes.com/2026/07/05/opinion/therapy-loneliness-friendship.html
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments