From the Editor
His suicidal thoughts were so strong that he had written a suicide note. Yet, during the months before we met in the ED, he had hesitated to seek care. As a doctor, he knew he had severe depression but he told me that he felt he couldn’t get help.
Such stories are all too common. In a CMAJ study, Dr. An Yi (Annie) Yu (of the University of Toronto) and her co-authors shed light on physicians’ seeking help for suicidality. They drew from the literature (literally): analyzing 52 narratives from academic papers, finding various barriers to seeking care, including aspects of medical culture, and identified facilitators, such as confidential services. “The pressure to achieve in medicine often discourages physicians from acknowledging their need for help, but the value of meaningful work emerged as a positive factor for mental health. The stigma regarding mental health concerns was substantially reduced through role modelling of help-seeking behaviour by colleagues.” We consider the study and its implications.
GLP-1 receptor agonists are having a moment because of the evidence for diabetes and other conditions. In the second selection, Nicholas C. Peiper (of the University of Louisville) and his co-authors focus on those with eating disorders, analyzing data to understand use and misuse in a new JAMA Psychiatry research letter. “This cross-sectional study found that GLP-1 RA use and misuse were common in a targeted sample of people with eating disorders.”
And in the third selection, from JAMA, Dr. Benjamin Chin-Yee (of Western University) writes about consult notes. He wonders what is lost in the “digital transformation” of templates and AI scribes. He worries about the future of the consult note. “The tools may evolve, but the art of pausing, thinking, and telling a story is still ours to preserve.”
DG
Selection 1: “A qualitative analysis of the barriers and facilitators to physicians and trainees seeking help for suicidality”
An Yi (Annie) Yu, Erene Stergiopoulos, Javeed Sukhera, et al.
CMAJ, 23 February 2026

Rates of physician suicide are relatively high compared with the general population and other professional fields. More than one-third of respondents of the 2021 National Physician Health Survey in Canada reported having thoughts of suicide at some point in their life, nearly doubling rates reported before the COVID-19 pandemic. Despite the increased prevalence of suicidal thoughts among physicians, limited studies have analyzed the nature of physician suicidality, especially for medical trainees. An American survey showed that physicians with suicidal thoughts are less likely to seek help for their mental health than their colleagues without such thoughts, even when those colleagues are also struggling with mental health challenges…
The development of supports that are accessible and acceptable for physicians requires a deeper understanding of their perceived experiences regarding seeking help, defined as any time a physician or trainee reaches out to another person, whether in professional or personal settings, to address their suicidality. Published narratives can provide insights and are one of the most accessible sources of data, given the profound stigma and pervasive fear of professional repercussions that deter physicians from openly disclosing suicidality. For physicians and medical trainees, a rich data set of narratives has been published in medical journals.
So begins a paper by Yu et al.
Here’s what they did:
- They conducted “a qualitative analysis of published narratives from physicians and trainees describing experiences in seeking help for suicidality.”
- They started by doing a systematic search of MEDLINE and PsycInfo from March 2000 to 2023.
- They then used reflexive thematic analysis to conduct a qualitative synthesis of the included narratives, an approach where “themes are constructed through ongoing reflexive engagement rather than passively emerging from the data.”
- They included physicians or trainees describing personal suicidality, help-seeking experiences, or experiences of losing a physician/trainee to suicide.
- The team was composed of members from different stages of residency training and clinical practice. “Several had experience with patients or family members manifesting suicidality…”
Here’s what they found:
- 347 articles were screened; 52 were included in the analysis.
- Backgrounds. About a third who experienced suicidal ideation or died by suicide were residents. Specialties included internal medicine (16.7%), surgery (9.3%), and psychiatry (7.4%). The self-reported diagnoses included depression (27.8%).
- Narrative structure and descriptions of suicidality. “All articles conveyed profound vulnerability through emotionally charged storytelling in either the first or third person. Authors described the process of seeking help or recounted tragic losses to suicide, collectively rallying the medical community to take urgent action to prevent suicide among ‘our own.’”
- Barriers. “Identified barriers to seeking help included the medical culture of stoicism, achievement, and value of professional identity; the growing severity of illness; stigma against mental health concerns; fear of burdening others; logistic challenges; and licensure concerns.”
- Facilitators. “Identified facilitators to seeking help included access to confidential services, mental health literacy, and care and role modelling. For authors who did seek help, they described accessing settings where they knew their stories would remain anonymous or confidential. These settings included both professional avenues and informal opportunities facilitated by colleagues, such as gatherings with strict confidentiality. Although meaningful connections were created in these settings, authors also reflected on how isolated and fearful physicians with suicidal thoughts can feel, as they resort to remote or indirect avenues to access support.”
Select quotations –
Descriptions of suicidality
“My work lost meaning; I was just going through the motions.”
“I didn’t know it then, but I had long experienced classic signs of burnout: emotional exhaustion, depersonalization, and low perceived personal achievement. But the burnout had been waxing and waning for 22 years; now I was in the worst episode of major depression of my life.”
“Yet my feeling of mastery came to an abrupt halt when I learned of the suicide of another friend and fellow medical student at the beginning of his third-year clerkships. His death hit me like a train.”
Barriers to help-seeking process
“Even as I held onto the love of my children and wife, my brain told me they would be better off without me.”
“I describe starting to use alcohol to medicate my anxiety, and the end, the moment when I knew I needed help.”
Facilitators to help-seeking process
“For the next 3 years, more than 40 students came to my home for support, friendship, and the opportunity to vent about the demands of medical school. It meant so much to me to know that I was not alone and that friends I admired had similar problems — it made me feel empowered rather than ashamed to take care of myself.”
“I told her I was sad that my 2-year-old niece wouldn’t remember me. ‘Do you think I would ever let her forget you?’ she responded. We both cried. She knows my depressions well: her unconventional response brought me back to reality.”
A few thoughts:
1. This is an excellent paper, offering insights into a real problem, and published in a solid journal.
2. The main finding in a sentence: “Intense pressures to achieve in medicine discourage physicians from acknowledging distress and seeking help, but role modelling of seeking help can attenuate the stigma.”
3. Dr. David Goldbloom – a co-author of this study – has commented that “the white coat is not Kevlar against the slings and arrows of outrageous fortune.” Well said.
4. There is something haunting and unsettling about this paper but, at the same time, hopeful.
5. Indeed, the paper includes thoughtful suggestions on supporting physicians and trainees:
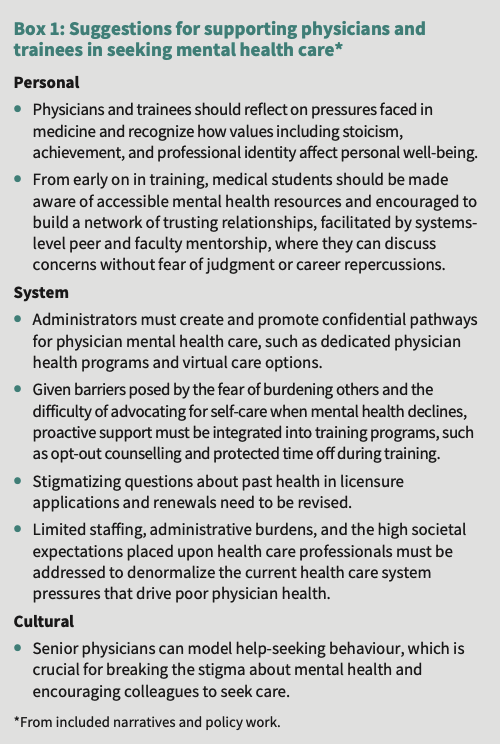
The suggestions for system change seem particularly thoughtful and important.
6. Past Readings have considered physician and trainee mental health. In a paper for JAMA, Dr. Rahael Gupta, then a medical student, discusses her experiences with depression. “Depression is not weakness, though depression is a disease that may make you feel weak. Depression is neither laziness, nor apathy, nor a lack of professional fortitude.” That Reading can be found here:
The full CMAJ paper can be found here:
https://www.cmaj.ca/content/198/7/E238
Selection 2: “Use and Misuse of GLP-1 Receptor Agonists Among People With Eating Disorders”
Nicholas C. Peiper, Jon E. Zibbell, Andrew S. LaJoie, et al.
JAMA Psychiatry, 24 June 2026 Online First

Emergent research suggests that people with eating disorders may be using and misusing glucagon-like peptide-1 receptor agonists (GLP-1 RAs) to maintain their eating disorders (eg, anorexia nervosa, bulimia nervosa, and binge eating disorder) through rapid dietary restriction and weight loss. Furthermore, recent shortages in commercial GLP-1 RAs have led to the proliferation of compounded and illicit products of unknown quality. To our knowledge, no studies to date have estimated GLP-1 RA use and misuse among people with eating disorders. This study evaluated the prevalence of GLP-1 RA use and misuse in a sample of people with eating disorders in the US.
So begins a research letter by Peiper et al.
Here’s what they did:
- They conducted an interim analysis of an ongoing cross-sectional study of US adults with eating disorders.
- Recruitment included “advertisements with national organizations and targeted outreach through online recruitment platforms.”
- They assessed lifetime and current use of GLP-1 receptor agonists, including commercial and compounded products, using survey questions adapted from validated drug use and mental health surveys.
- “Misuse included use of a commercial or compounded product by taking more than the prescribed starting, titration, or maintenance dose; increasing the dose before prescribed; taking less than the prescribed dose; taking for a longer period than prescribed; disassembling or tampering with the injection equipment; or sharing with family, friends, or acquaintances without a prescription.”
Here’s what they found:
- 557 individuals completed the study screener; 436 met eligibility criteria and passed quality control checks.
- Demographics. The mean age of participants was 34.1 years; the vast majority were female (94.2%); most were White (88.5%).
- Completion. “Item-level missingness was low (≤2%).”
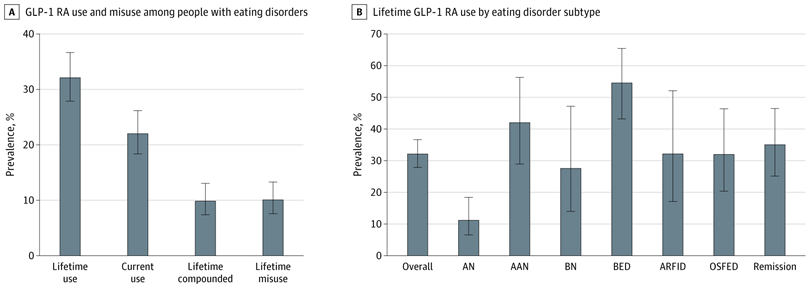
- Use. A total of 140 individuals (32.1%) reported lifetime GLP-1 RA use and 96 (22.0%) reported current use.
- Misuse. The prevalence of lifetime misuse was 10.1% and of lifetime use of compounded products was 9.9%. (!)
- Eating disorders. Lifetime GLP-1 receptor agonist use was most common among participants with binge eating disorder and atypical anorexia nervosa. See the graph below.
A few thoughts:
1. This is a good letter, offering early data.
2. The main finding in a sentence: many used GLP-1 RAs (about a third of those with eating disorders over their lifetime) and some misused (about one in 10).
3. Ouch.
4. As the authors observe: “There are no indications for any eating disorders.” They add: “People with eating disorders are also navigating a rapidly evolving risk environment of compounded GLP-1 RAs that are easily obtained without medical or regulatory oversight.”
5. Like all studies, there are limitations. The authors note several, including: the reliance on self-reporting.
The full JAMA Psychiatry research letter can be found here:
https://jamanetwork.com/journals/jamapsychiatry/article-abstract/2850584
Selection 3: “The Death of the Consult Note”
Benjamin Chin-Yee
JAMA, 10 March 2026

My hospital is finally phasing out human transcription. I’ll admit, relying on a person to decode my ramblings, to sift ‘ums’ and spell out acronyms amid background chatter and overhead alarms, feels archaic. In an age when we dictate shopping lists to our phones and ask artificial intelligence (AI) chatbots for parenting advice, manual transcription seems a relic of a bygone era.
So begins a paper by Dr. Chin-Yee.
He talks about learning to dictate notes. “I still remember the awkwardness of learning to dictate early in my medical career. For years, I struggled to dictate in front of others, retreating to a quiet nursing station or vacant call room while I tried to process the patient encounter. I’d press the phone tightly to my ear and speak slowly and softly, praying no one would hear me.”
He recognizes the importance of the process. “What I didn’t appreciate then – but understand now – is that this discomfort was not a flaw in the process. Rather, it was the process.” He adds: “Dictation forced me to gather my messy, scattered thoughts and shape them into a story. It forced me to make choices about what mattered, to hear the logic of a case spoken in my own voice. It was clinical reasoning in action.”
He notes templated notes and growing patient volume. “In this environment, documentation feels peripheral to the real work of doctoring. The result is a note that is quick, efficient – and wholly unremarkable.”
He speaks of notes. “There was a time when reading a seasoned consultant’s note felt like being guided through their reasoning – an elegant arc punctuated by astute observation, rising through a crisp differential, and culminating in coherent synthesis – all with distinctive flair. What it lacked in data, it more than made up for in meaning. Now, our eyes glaze over at the sight of endless lists and prefabricated blocks of text, the narrative drowned beneath a rising tide of autopopulated content.”
The contrast with today is sharp. “Today, trainees are spared the fear of a blank page, starting instead with a screen half-filled.” Is this really progress? “Medicine has always been in the business of sense making – turning symptoms into stories, information into insight. Dictation offered a natural pause for that work, a moment to gather one’s thoughts and hear one’s own reasoning aloud. Optimists might argue that nothing prevents us from doing the same now, simply dictating to an algorithm instead of a person. But as speech-to-text dictation becomes embedded within templated workflows and as newer tools like automated scribes and ambient AI ‘listen’ and draft notes in the background, the mental work of shaping a narrative subtly slips away. What fades is not just the human transcriptionist but the type of thinking the human transcriptionist once required.”
He recognizes that times have changed. “Templates and AI are here to stay. They solve real problems for overburdened clinicians working in an overstretched system. Some tools may even open new spaces for reflection; some hope ambient AI will capture the patient’s story while freeing the clinician to share their reasoning aloud at the bedside.” He is realistic. “Railing against the tides of technology may be futile.” He is also thoughtful. “But preserving the cognitive pause that dictation demanded is not. Even in an era of templated notes, we can still teach trainees to voice their assessments before they document: to treat the Impression not as a box to complete but as space for making sense of everything that came before. We can also safeguard the remaining arenas where reasoning still happens in real time, such as morning report, oral case presentations, or clinical rounds.”
“Because a consult note is, at its core, a form of storytelling – an attempt to give shape to uncertainty, to show what makes sense and what does not. Dictation once helped that work along, forcing the clinician to select details, impose order, and listen aloud to their own reasoning. The question now is whether we will continue to see ourselves as storytellers and sense makers or hand that work to systems that document flawlessly yet illuminate nothing.”
A few thoughts:
1. This is a solid paper.
2. In a world where paperwork is viewed as burdensome, EMRs and AI seem like a positive development. But the author asks about what we are losing in the process.
3. Let’s not be overly nostalgic for the past (and the long hours of charting). But let’s also not replace the quiet beauty of an eloquent note with the Pablum of AI.
The full JAMA paper can be found here:
https://jamanetwork.com/journals/jama/article-abstract/2844543
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments