From the Editor
In the year before they suicide, more than 90% of people have had contact with some type of acute care – an ED visit, a trip to the family doctor, or an appointment at an outpatient specialty clinic. So how can we help people better? Given the contact, what can we do to reduce suicides?
This week, we have two selections; the first focuses on this question. In a new JAMA Psychiatry paper, Dr. Stephanie K. Doupnik (of the University of Pennsylvania) and her co-authors do a systematic review and meta-analysis of 14 studies that used brief suicide prevention interventions in acute care settings (think brief contact interventions like a phone call after an ED visit). They find an encouraging result: “In this meta-analysis, brief suicide prevention interventions were associated with reduced subsequent suicide attempts.” We consider the big paper, and the editorial that accompanies it.

In the other selection, therapist Lori Gottlieb discusses race and therapy in a Washington Post essay. She examines her own biases, and the way they play out in her therapy session. “Here’s what we didn’t talk about [in school]: the racism that might take place inside the supposedly ‘safe space’ of our therapy rooms – our patients’ racism and our own.”
Please note that there will be no Reading next week. Happy Canada Day.
DG
Selection 1: “Association of Suicide Prevention Interventions With Subsequent Suicide Attempts, Linkage to Follow-up Care, and Depression Symptoms for Acute Care Settings: A Systematic Review and Meta-analysis”
Stephanie K. Doupnik, Brittany Rudd, Timothy Schmutte, et al.
JAMA Psychiatry, 17 June 2020 Online First
![]()
Suicide rates have been rising for 2 decades in the US. In response to this crisis, the National Action Alliance for Suicide Prevention has called for health care organizations to incorporate suicide prevention into routine practice. Health care organizations are well positioned to prevent suicide deaths because more than one-third of people who die by suicide have a health care encounter in the week before their death and half within a month before their death…
Brief interventions are used in acute care to identify and provide initial management for a number of mental health and other problems and offer several practical advantages. Brief interventions can be delivered in a single time-limited encounter by trained professionals and include an emphasis on ongoing treatment…
To establish evidence for brief acute care suicide prevention interventions, we conducted a systematic review of clinical trials of brief suicide prevention interventions delivered in a single in-person encounter (in some cases, with telephone follow-up) that directly addressed suicide risk, promoted continuity of mental health care, or both.
So begins a new paper by Doupnik et al.
Here’s what they did:
- They searched several databases, including Scopus; papers were included if they were published between 1 January 2000 and 31 December 2019.
- Studies describing clinical trials of single in-person encounters were included.
- The interventions: safety planning, brief contact interventions, coordination of care, and other brief interventions. For example, brief contact interventions “include telephone calls, postcards, and letters…”
- Two reviewers independently extracted data (following PRISMA guidelines).
- The primary outcomes included subsequent suicide attempts, linkage to follow-up care, and depressive symptoms at follow-up.
Here’s what they found:
- A total of 14 studies were included, representing 4 270 patients. Brief contact interventions were part of the suicide interventions found in 6 of the 14 studies – but ranged from one appointment reminder to 11 texts over a full year.
- 7 studies measured attempts; 9 studies considered follow-ups; 6 studies looked at depressive symptoms. Forest plots of the outcomes follow.
- Pooled-effect estimates showed that brief suicide prevention interventions were associated with reduced subsequent suicide attempts (pooled odds ratio, 0.69), and increased linkage to follow-up (pooled odds ratio, 3.04)
- They were not associated with reduced depression symptoms (Hedges g = 0.28).
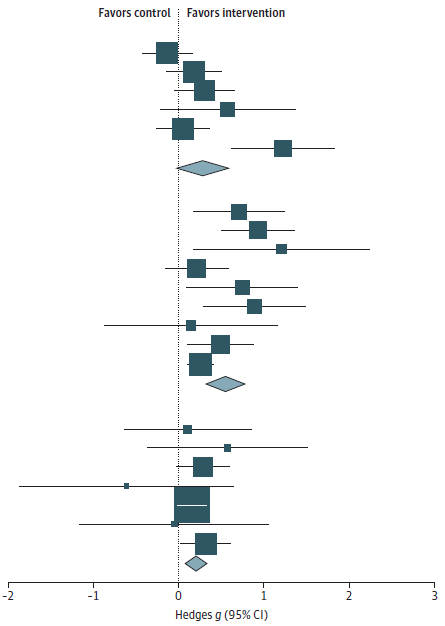
Meta-analyses showed that the pooled effect of the interventions was to reduce subsequent suicide attempts and increase linkage to follow-up care. Reduction in depression symptoms at follow-up was not statistically significant.
A few thoughts:
- This is an important paper.
- This is a hopeful paper.
- The authors are bold in their findings. The boldest: they estimate that there were 78 fewer attempts in the 2 241 patients who were included in the analysis of this outcome, a reduction of 3.5%.
- The paper only included brief preventive interventions. What if the interventions had been more sophisticated and included more intensive care for those at higher risk?
- This study is a well done, drawing on 14 studies with clearly defined interventions. But a few words of caution: individual studies varied greatly in the way that interventions were conducted; returning to brief contact interventions, note (again) that they ranged from one appointment reminder to multiple texts over 12 months. And we must acknowledge that the causes of suicide are complex and multidimensional, making it challenging to compare an intervention in one clinical situation with another.
- The paper runs with a commentary.
“Do Brief Preventive Interventions for Patients at Suicide Risk Work?”
Nadine M. Melhem and David Brent
Melhem and Dr. Brent (both of the University of Pittsburgh) see the urgency of the situation, noting that many people who suicide have had a health care contact before – almost a third have had that contact in the week prior to suicide. “Thus, the need for effective brief interventions that could be easily applied by a range of clinicians at each one of these settings to reduce risk for suicide is now more important than ever.”
They see much to like in the Doupnik et al. meta-analysis. They note the importance of the task, especially with regard to helping people follow-up with care: “Studies report only 35% of adult hospital discharges keep an outpatient appointment within 7 days of discharge, and 55% keep an outpatient appointment within 30 days.”
Reviewing the findings of the meta-analysis, they argue for a more comprehensive approach: “A combination of these approaches is likely needed for the long-term reduction in risk for suicide. It is important to note that this meta-analysis did not include several brief interventions that may have required more than a single encounter but are also promising in reducing risk for suicidal behavior and could work in other types of settings.”
And they favour more experimentation and research. They also favour efforts to reduce stigma:
However, before delivering an intervention, we need to first embrace as a medical community the widespread screening for suicidal ideation to identify those at risk. We cannot continue to inadvertently apply the ‘don’t ask’ mindset in our health care systems. We need to break the stigma and the discomfort about asking questions related to suicidal ideation and behavior, which originate from the lack of training and preparedness about the next steps after identification.
A final thought: the last comment is striking.
The commentary can be found here: https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2767406
The Doupnik et al. paper is here:
https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2767408
Selection 2: “I thought I was an antiracist therapist. Then I looked more closely.”
Lori Gottlieb
Washington Post, 18 June 2020
![]()
Over the past few weeks, since George Floyd’s killing in Minneapolis police custody galvanized conversations about racism across the globe, conversations have been taking place among mental health practitioners. We’ve been discussing the emotions that our patients have been bringing up in sessions – the anger and sadness and grief. But we’ve also been discussing what’s come up for us, the clinicians.
Of all the professions associated with racism, therapy probably isn’t what first comes to mind. Therapy is a healing profession that self-selects for compassionate people who have a deep interest in illuminating rather than suppressing uncomfortable truths. But what happens if mental health practitioners aren’t aware of their own discomfort with the topic of race? We’re supposed to be the profession where nothing gets swept under the rug, but are we complicit in doing just that?
So begins an essay by Gottlieb, a psychotherapist. She wrote an essay recently about psychotherapy and the toilet as the new couch (considered in a past Reading). Here, she is more sober. She notes her training, and the emphasis on considering her own background and biases. She also notes the consideration of discrimination: “We discussed the ways in which race, gender, age, sexual orientation, religion and socioeconomic status subject people to discrimination – and, in turn, depression, anxiety and trauma.”
But she wonders about the way she handles race issues:
An example: A white patient is telling me a story about being afraid while walking to her car on a deserted street because there was ‘a black man’ standing nearby. She had been raped two years earlier on a deserted street – by a white man. I wonder why this man’s skin color matters, and I want to say something like, ‘Tell me why you mentioned that he was black.’ But I don’t, and I justify it to myself by thinking that I shouldn’t interrupt her story while she’s crying, or that my saying this might sound judgmental. But I also know that if I were a therapist committed to racial equity, I would have asked.
A few thoughts:
- Some will find these comments important, a commitment to racial equity. Others may be cooler.
- But I suspect many will feel that her concluding comment is thoughtful: “There’s a world of difference between the so-called cultural competence that we were taught in graduate school and cultural humility, which is a deep curiosity about our patients’ experiences, an ability to bear witness to the truth of their lives and a keen awareness that we have work to do if we want to be therapists who are part of the change that our patients – and society – so desperately needs.”
- What to read given the moment? A colleague suggests “White Academia: Do Better.” This short essay by Jasmine Roberts (of the Ohio State University) is cutting, sharp, and incredibly relevant. She pushes much further than Gottlieb. Her list of ten actions may be considered essential reading.
The essay can be found here: https://medium.com/the-faculty/white-academia-do-better-fa96cede1fc5
The Washington Post article is here: https://www.washingtonpost.com/opinions/2020/06/18/i-thought-i-was-an-antiracist-therapist-then-i-looked-more-closely/
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments