From the Editor
Canada’s Parliament is debating a ban. Government officials are discussing similar measures in the UK, Poland, Denmark, and Malaysia. As more and more countries think about restricting kids from access to social media, the Australian experiment is interesting and important. In 2024, Australia passed legislation banning youth under the age of 16 years.
But has the Australian law had an effect on use? In The BMJ, Courtney Barnes (of the University of Newcastle) and her co-authors attempt to answer that question with a prospective observational study. They analyzed survey data collected just before implementation and again three months after it, involving 408 youth. “Despite the intent of the Social Media Minimum Age Act 2024 to delay access to social media platforms and reduce the potential for online harms, little evidence was found of immediate substantive reductions in reported social media use by adolescents under 16 years.” We consider the study and its implications.

In the second selection, Maiara da Silva Martins (of Pontifical Catholic University of Rio Grande do Sul) and her co-authors focus on cellphone restriction in Brazil during the school day. In a letter published in Journal of the American Academy of Child & Adolescent Psychiatry, they report on a longitudinal study involving 1 643 students. “Our findings suggest that school-hour restrictions alone are insufficient to alter the trajectory of internalizing problems like anxiety and withdrawal.”
And in the third selection, from The Canadian Journal of Psychiatry, Dr. Colin M. Shapiro (of the University of Toronto) and his colleagues write about sexsomnia. They note that the condition is more common than previously believed and offer some clinical tips. “For clinicians, the key point is that sexual behaviours during sleep can occur without conscious awareness and should be considered within the broader spectrum of parasomnias during clinical assessment.”
DG
Selection 1: “Assessing early effects of Australia’s Social Media Minimum Age Act on adolescents’ social media use: observational study”
Courtney Barnes, Alix Hall, Stephanie Mantach, et al.
The BMJ, 24 June 2026 Online First
Adolescents are highly digitally connected, with use of social media platforms embedded in their daily routines. Globally, adolescents spend increasing amounts of time on platforms such as TikTok, Instagram, Snapchat, and YouTube, often accessing multiple platforms each day and across several devices. In England and Australia, more than 90% of children aged 13-18 years report using social media, often for more than three hours a day…
Digital media environments, including social media, provide adolescents with opportunities for connection, self-expression, and access to information and can support social development and the maintenance of peer relationships. Social media may also allow young people to explore interests, access educational content, and engage with supportive online communities. However, some patterns of adolescents’ social media use, including excessive or unregulated use, may have negative effects on adolescents’ health and wellbeing, including increased psychological distress (for example, symptoms of anxiety and depression), poorer sleep (for example, later bedtimes and reduced sleep duration), and other factors that contribute to broader concerns about adolescents’ physical and mental health.
Australia implemented a world first regulatory reform targeting social media platforms in late 2025: the Online Safety Amendment (Social Media Minimum Age) Act 2024… The Act established a national minimum age of 16 years for holding accounts on 10 designated social media platforms including TikTok, Instagram, and Snapchat. Under the Act, these platforms must take reasonable steps to prevent users under 16 from creating or maintaining accounts, including through age assurance measures.
So begins a paper by Barnes et al.
Here’s what they did:
- They conducted a prospective observational study to “examine the early effect of a world first national policy (Social Media Minimum Age Act 2024), which established a national minimum age of 16 years for holding accounts on designated social media platforms…” They surveyed adolescents immediately before implementation and again three months later.
- They used several strategies to recruit participants, including social media advertisements, contacting parents who had previously participated in trials, and website promotions.
- They included Australian adolescents aged between 12 and <17 years at the time of implementation of the age restrictions.
- Participants completed online questionnaires assessing social media access, frequency of use, time spent on social media, platforms used, exposure to age-verification measures, and attempts to circumvent restrictions.
- The primary outcomes: daily social media use and time spent using social media.
- They used different statistical analyses, including a sharp regression discontinuity design comparing adolescents just below and just above the age threshold created by the legislation. This quasi-experimental approach aimed to isolate the association between exposure to the Act and social media use while minimizing confounding.
Here’s what they found:
- 436 adolescents were included. Of these, 408 participants completed the follow-up survey; the retention rate was 94%.
- Demographics. Participants had a mean age of 14.33 years and the majority (54%) were female. Most (67%) were recruited from New South Wales, Australia, and lived in big cities (84%).
- Use. “More than 85% of participants aged under 16 years reported using social media platforms subject to the Act at follow-up, predominately via use of their own accounts (54-68%)”. While about two-thirds encountered age-verification measures, relatively few were required to provide government-issued identification, and 15-19% reported using fake accounts to bypass restrictions.
- Daily use. “Between baseline and follow-up, daily social media use was stable among 12-13 year olds; reduced somewhat among those aged 14-15 years (from 78% to 69%); and increased for those aged >16 years (from 80% to 89%).”
- Time. “Time spent per day using social media was relatively stable between baseline and follow-up for 12-13 year olds and those aged >16 years but was lower at follow-up for those aged 14-15 years (from 3.40 to 3.13 units on an ordinal scale).”
- Analysis. “In regression discontinuity design analyses, insufficient evidence was available to support a discontinuity in social media use on these primary outcomes (P≥0.60).”
A few thoughts:
1. This is a good paper offering data on a relevant question, and published in a major journal.
2. A four-word summary of the study: the legislation didn’t work.
3. Do Australians need to wait longer to see change? Cultural change often takes time, after all – but the problem appears to be different: youth simply ignored the new rules. More than 85% of adolescents under 16 continued to use platforms at three months’ follow-up, mainly through their own accounts. Though the majority were asked their age, the survey suggests that many youths provided false information (more than one in four provided a self-declared age). Others used fake accounts or accessed social media through private browsers. Australia may be a case study in how not to implement a ban.
4. What would be an alternative? The BMJ also includes a commentary paper by Andy Burrows (of the Molly Rose Foundation). He writes:
“A more effective approach would be to insist that tech platforms follow stringent product safety standards and explicit safety-by-design requirements as a precondition of entry to the UK market. Regulatory regimes need the power and risk appetite to reset the incentives for some of the largest, richest companies in the world.”

Andy Burrows
That paper can be found here:
https://www.bmj.com/content/393/bmj-2026-100046
5. Like all studies, there are limitations. The authors note several, including: “the reliance on self-reported measures to assess adolescents’ social media use is a considerable methodological limitation of the study.”
The full BMJ paper can be found here:
https://www.bmj.com/content/393/bmj-2026-363695
Selection 2: “Problematic Smartphone Use and Mental Health Trajectories During Brazil’s First-Year School-Hour Restrictions”
Maiara da Silva Martins, Victor Matheus Lopes Martinez, Thiago Wendt Viola,
Journal of the American Academy of Child & Adolescent Psychiatry, 16 June 2026 Online First
Smartphones can facilitate communication and access to information. However, excessive use has been associated with poorer mental health among children and adolescents. Recent longitudinal evidence suggests that earlier smartphone acquisition and high frequency of use are linked to increased internalizing and externalizing symptoms in early adolescence. In response, multiple education systems have implemented restrictions on in-school smartphone use.
In Brazil, Federal Law No. 15,100 (January 13, 2025) regulates students’ use of portable electronic devices in basic education and restricts use during school activities. The primary objective of this legislation is to safeguard the mental, physical, and psychological health of children and adolescents by reducing digital distractions during pedagogical time.
So begins a letter by Martins et al.
Here’s what they did:
- They conducted “a three-wave school-based longitudinal study in public and private schools in southern Brazil” to examine mental health trajectories during the first academic year after the introduction of restrictions on smartphone use during school hours.
- “The waves were timed by the academic calendar: Wave 1 in March (baseline, start of the school year), Wave 2 in June (mid-year, 3 months post-baseline), and Wave 3 in October (end of the school year, 7 months post-baseline).”
- At each assessment, students completed the Smartphone Addiction Scale–Short Version (SAS-SV) which was used to identify problematic smartphone use (SPU). Students were classified as being at risk for SPU based on their baseline score.
- Emotional and behavioral functioning was assessed at each wave using the Strengths and Difficulties Questionnaire (SDQ).
- Primary outcomes: total difficulties, externalizing symptoms, internalizing symptoms, and prosocial behavior.
- Different statistical analyses were done, including mixed-effects regression models to examine changes in mental health over time among students with and without baseline SPU, adjusting for age, sex, and school type.
Here’s what they found:
- 1 643 students were included. 1 429 students (87%) completed the final assessment seven months later.
- Demographics and SPU. Participants had a mean age of 13.2 years; 48.5% were female; approximately one-third (32%) met criteria for SPU at baseline.
- Prevalence. The prevalence of SPU remained stable throughout the study (32% in March, 32% in June, and 30% in October).
- Difficulties. Across all three assessments, students at risk of SPU had significantly higher levels of emotional and behavioral difficulties than their peers (all p<0.001). They reported higher total difficulties, externalizing symptoms, and internalizing symptoms, although prosocial behavior did not differ between groups.
- After restrictions. Adolescents at risk for SPU experienced small reductions in total difficulties and externalizing symptoms, particularly conduct problems.
A few thoughts:
1. This is a solid letter providing early data.
2. The main findings in a sentence: the prevalence of SPU didn’t change but those at risk had fewer difficulties. (At best, a mixed picture.)
3. Some perspective: improvements were very small for those at risk (Cohen’s d=0.07 for total difficulties), and no significant improvements were observed for internalizing symptoms or prosocial behavior.
4. Of course, these results are after just one year.
5. Still, restricting smartphone use produced minimal benefits.
The full Journal of the American Academy of Child & Adolescent Psychiatry letter can be found here:
https://www.jaacap.org/article/S0890-8567(26)00267-4/fulltext
Selection 3: “Sexsomnia: A Clinical Entity Psychiatrists Should Know About”
Colin M. Shapiro, Julian A. Gojer, Chris Y. Kim
The Canadian Journal of Psychiatry, 16 June 2026 Online First

In a review titled “Forensic Evaluation of Sexsomnia” published in the Journal of the American Academy of Psychiatry and the Law, approximately half of the 27 cited articles explicitly included the term ‘sexsomnia’ in their titles. This suggests that since we first described the phenomenon in the Canadian Journal of Psychiatry, sexsomnia has become increasingly recognized as a legitimate clinical entity.
A recent self-reported survey suggests that the condition may be more common than previously believed, with reported lifetime prevalence of approximately 7.1% to 10.1% and a current (past 3 months) prevalence of 6.1%. Public awareness has also expanded beyond medical literature and sexsomnia was also featured in an episode of the popular medical drama, House, M.D.
Awareness of the condition is increasing, but sexsomnia may still be overlooked by clinicians.
So begins a paper by Shapiro et al.
- The definition. “It is generally conceptualized as a subtype of non-rapid eye movement (NREM) parasomnia, a form of arousal such as sleepwalking. In the Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition-Text Revision, these disorders are characterized by incomplete arousal from deep sleep accompanied by complex behaviours occurring without full awareness.”
- The literature. “The forensic literature describes a wide range of behaviours, including non-consensual sexual contact, masturbation and penetrative sexual activity while asleep.”
- The distinction. “Sexsomnia is generally considered to arise from a primary sleep disorder rather than from paraphilic interests or other primary sexual disorders… Sexsomnia can be conceptualized within this broader family of parasomnia disorders.”
- The differential. “Sleep-related epilepsy features highly stereotyped, often sudden, brief and repetitive motor seizures, while REM behaviour disorder occurs during late-night REM sleep, presents with vivid dream-enactment and primarily affects older adults.4 In contrast, substance-induced disinhibition, dissociative states, active psychosis/mania, paraphilic disorders and malingering are distinguished by preserved conscious awareness, distinct daytime psychiatric symptoms or clear volitional motives.”
They note the chronic course and, as a result, a possible “significant relationship strain and (in some circumstances) legal issues. Individuals may face accusations of sexual assault or non-consensual sexual behaviour during sleep, which may lead to legal charges and forensic evaluations.” More: “In a 2019 review of 351 forensic referrals to a sleep centre, 41% were related to allegations of sexual assault. Of these, 110 cases were accepted for forensic sleep evaluation after excluding cases better explained by other medical or psychiatric conditions, alcohol intoxication or illicit drug use. Sexsomnia was the most frequent diagnosis in this population. None of the evaluated cases was thought to be malingering.”
They note the legal issue. “If a sexual interaction is non-consensual and the individual is awake, it constitutes sexual assault. When the active partner is genuinely asleep, the behaviour may be considered non-volitional. In many jurisdictions, this can mean the individual is not held criminally responsible. A central challenge in such cases is determining whether the individual was truly asleep or whether sleep is being claimed to avoid culpability.”
A couple of thoughts:
1. This is a helpful and reasonable paper (part of the Clinician’s Corner series).
2. How then to approach such patients? They suggest a clinical workflow:
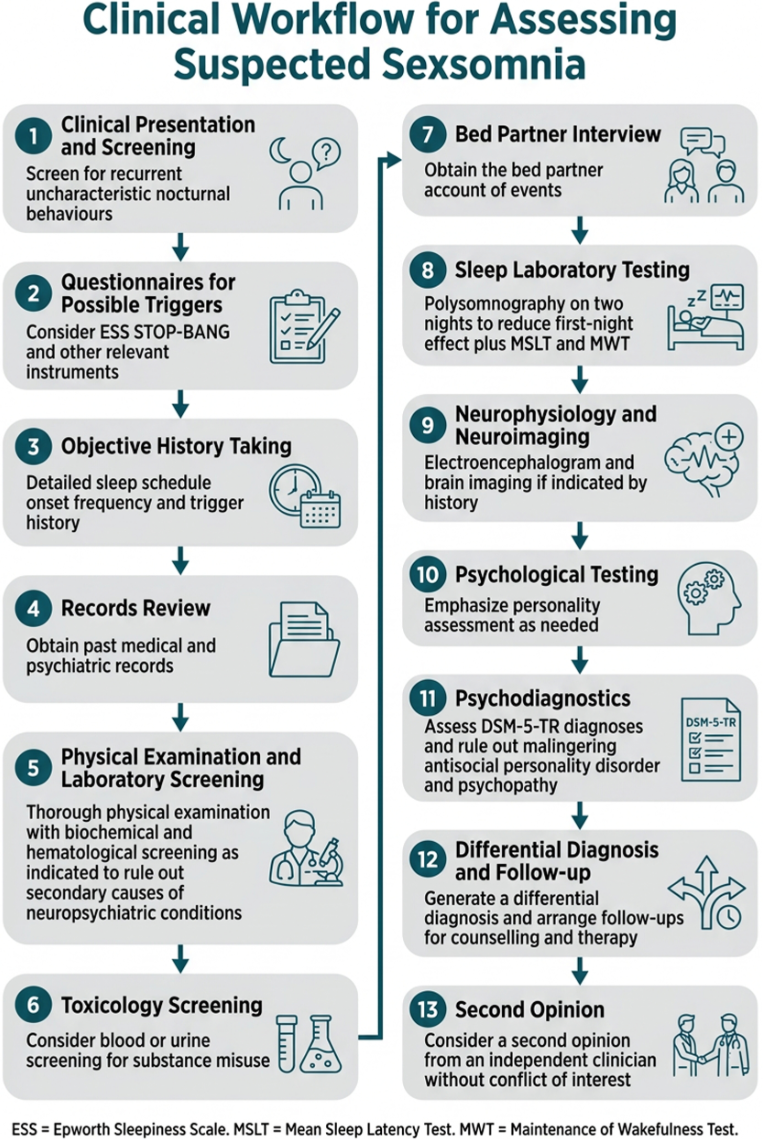
The full Canadian Journal of Psychiatry paper can be found here:
https://journals.sagepub.com/doi/full/10.1177/07067437261458523
Reading of the Week. Every week I pick articles and papers from the world of Psychiatry.
Recent Comments